Understanding Toxoplasma gondii: Parasitic Infection and Human Health Impact
- 10 Pages
- Published On: 25-05-2024
Introduction
Toxoplasma gondii is an intestinal coccidium that parasitizes on members of the cat family and is considered as the most successful pathogen. Its primary asymptomatic infection is commonly in humans. In addition, over 30 percent of the human population endures chronic toxoplasmosis infection. Toxoplasmosis has been researched to be included as one of the most common parasitic infections that affects both man and a number of other warm- blooded animals. The probable primary infection in individuals is mostly lymphadenopathy or ocular toxoplasmosis but severe toxoplasmosis may occur in immunocompetent persons when infected with isolates like genotype 86 of T.gondii (Basit, Nasir, Vohra and Shazlee, 2018). For those studying this area, biomedical science dissertation help can provide valuable support. However, most affected individuals are not even aware of the infections since the infection is asymptomatic in its incubation period.

Reinfection of a latent infection in immunocompromised victims may cause toxoplasmosis encephalitis besides being at risk of chronic infection reactivation (Liu, Wang, Huang and Zhu 2015). Nevertheless, human toxoplasma infection depends on the strength of a person’s immune system. Notably, incidences of severe disease are often seen in congenitally infected children and in immunocompromised individuals, particularly patients with Acquired Immune Deficiency Syndrome (AIDS). A wide spectrum of diseases caused by the parasite, particularly, toxoplasmosis can be visible in affected children. Mild occurrences may utterly depict symptoms such as diminished vision but in instances of severe infection, various chromosomal deformations may be seen.
Medicinally, Toxoplasma antibody tests are always done to determine a past or current infection of toxoplasmosis. The antibodies IgG and IgM tests are conducted in tube of blood samples and an evaluation presented. (Liu, Wang, Huang and Zhu 2015) That is, a serological test is often used as a diagnosis to determine the seroprevalence of an infected person. Moreover, the serological tests estimate reactivation risks, preventive measure in immunocompetent persons, and claim an appropriate clinical follow up based on clinical context.
Evaluation of toxoplasma IgG and IgM test results
A negative toxoplasma IgG indicates no past infections and the patient has no immunity to toxoplasma infection.
Positive toxoplasma IgG indicates an active immunity to toxoplasma parasite.
Negative toxoplasma IgM means that there is no current toxoplasma infection.
Positive toxoplasma IgM presents a recent toxoplasma infection.
Discussion
Toxoplasmosis infection among immunocompromised individuals is majorly due to a reactivation of a chronic infection as a consequent of the progressive loss of cellular immunity. Toxoplasma encephalitis mainly develops when the CD4 cell count is below 100/mm3 hence its prevalence is directly proportional to the pervasiveness of antibodies to Toxoplasma in a population (Kodym et al 2015). For instance, in a population where 10 percent to 40 percent of individuals are HIV infected, a third of these population is likely to be susceptible to Toxoplasma encephalitis. However, it is not clearly estimated whether more than a third of these seropositive patients in such a population will develop Toxoplasmosis.
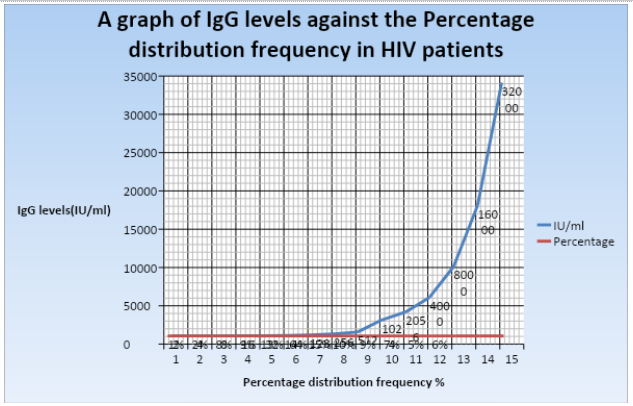
During the HIV infection, the antibody gene coding processes of CD4+ cells is very low as compared to the rapid antigen replication in HIV virus (Kodym et al 2015). The pathogen takes over CD4+ T cells and uses them for their replication thus depleting them, which compromises cytokine and chemokine secretion hence a significant decrease in immune response to antigens leading to thriving of opportunistic diseases or reactivation in instances of chronic infections (Robert-Gangneux and Belaz, 2016). In this regard, the levels of the IgG antibodies in the patients’ serum are likely to be high to initiate cell- mediated immunity at the first stages of infection. Regardless, these levels decrease as the HIV infection progresses thus patients present a negative toxoplasma IgG test. For instance, in graph 2 the distribution frequency percentage representing the HIV patients population against their IgG levels shows a significant rise in the patients’ IgG levels, which progressively decreases after two or three months of no medical attention. According to Kodym et al (2015) seronegative patients tend to develop acute toxoplasmosis at the onset of infection. Once an immune privileged subject is exposed to Toxoplasma gondii antigens he or she experiences seroconversion thus becomes seropositive. This activate antibody production hence the high IgG levels up to optimum level. That is to say, after infection the invasive form of the parasite, tachyzoites, infects nucleated cells and multiply thus destroying cells while producing necrotic foci embodied in inflammations. This triggers cell-mediated immunity from the T-cells, macrophages, and the type 1 cytokines, particularly interleukin-12 and interferon-gamma thus production of antibodies, which is reflected in high IgG levels (Kodym et al 2015). Antigen presenting cells produce interleukin-12 that stimulates the production of interferon-gamma, an antibody mediator that inhibits intracellular pathogenicity (Rougier, Montoya and Peyron, 2017). Besides, interferon-gamma further stimulates anti-T gondii activity both from macrophages and non-phagocytic cells. In addition, TNF-alpha, a cytokine is also produced to control the toxoplasmosis infection (Bharti et al., 2016). Furthermore, the CD8 derived from IFN-Y prevents further parasite multiplication and maintain the encysted parasite as a bradyzoite. Similarly, natural killer cells compensate for the absence of T-cells against Toxoplasma gondii in an immunocompromised patient (Bharti et al., 2016). As such, continued stimulation of antibody production maintains a latency of chronic T. gondii infection. Therefore, a continuous reactivation of the disease also continuously boosts the antibody levels as is shown in the below exponential curve. However; the onset of cell-mediated immunity against tachyzoites stimulates a transformation of the parasite into tissue cysts that escape immunity hence a later decrease in IgG levels (Rougier, Montoya and Peyron, 2017). Moreover, CD4 cell destruction by the HIV virus and a decreased vitro production of interleukin-12 and interferon-gamma facilitates the development of Toxoplasmosis in HIV patients. In this essence, a gradual impairment on both the cell mediated immunity and humoral response in immunocompromised victims tends to be weaker with time, which explains lower reactivation percentage of 2 to 6 percent in seroconversion entities (Bharti et al., 2016).
Research literatures affirm incidences of reactivated T. gondii infection in HIV patients causing high levels of antibody production in two months, IgG (ELISA). A prime example, in Denmark an overall cumulative incidence of 8 percent in AIDS patients was confirmed and France reported an incidence reactivation rate of 12 percent in HIV victims with Toxoplasma gondii acute infection. In a study, the monitored reactivation period of Toxoplasma gondii infection was registered to be 4.5 percent in males and 2.6 percent in females. Furthermore, an approximation of this incidence in critically immunocompromised patients with a CD4 cell count lower that 50/ul, the reactivation is likely to be within a 17.7 percent range or less (Kodym et al 2015). Similarly, the data in this study registers a reactivation incidence of 13 percent in relation to the total tested population of 18410 and a mean of 573.4. Consequently, our data can be used to assume that such patients were infected for a long period and may probably represent the one third groups of patients who registered a declining antibody trend.
Statistical evidence indicates that there is a significant difference in the levels of IgG antibodies of both immunocompetent and immunocompromised patient samples. Firstly, the median of these groups describe a varied difference hence statistically different. That is, the median value for the HIV infected patients is 125 and 32 for immunocompetent patients. Research suggests that a median value estimates the probability of how low of high a data set ranges to its typical form (Villard et al., 2016). In this regard, the high median value indicates the high seroprevalence among HIV –infected patients since their IgG levels lay within the 125 IU/ml, which is a boosted range as compared to those of the normal patients, 32 IU/ml and are seropositive. Moreover, the high standard deviation of 1342.4 for immunocompromised blood samples supports their extra-ordinarily boosted IgG levels during toxoplasmosis reactivation infections.
The rapid increase in the levels of IgG in immune-privileged patients shows that the IgG levels increase to prevent the individuals from invasiveness of the infection with Toxoplasma gondii. Also, the assumption that these two groups presented contrasting results evidently explains how their genetic makeup had a key role to play in the resistance during the infection period. They are genotypically resistant to Toxoplasmosis hence the reduction of their risks of contracting the infection.
Seroprevalence and IgG levels in patients with toxoplasmosis is determined by a variety of factors depending on climatic conditions in the habitats of the sample patients and their rate of exposure to coccidians, especially cats.
According to the graph showing the distribution frequency between the immunocompetent patients and their IgG levels, out of the 92101 immune privileged individuals only people with a distribution frequency of 1-24% diagnosed a rapid increase in the IgG levels; nevertheless, this is not as high as the levels recorded in HIV patients. The remaining 70865 healthy patient samples had low levels of IgG. These demographics further clarify the lower seroprevalence in immunocompetent subjects since the patients’ samples reveal insignificant levels of IgG.
On the other hand, seropositive entities presented significantly differently assumptions in relation to their immunocompromised samples. As earlier noted, a positive toxoplasma IgG reflects an active immunity towards toxoplasmosis; in this way, immunocompetent patients. Statistically, reactivation can occur in seropositive patients thus leading to retinochoroiditis. According to Kodym et al 2015) during toxoplasmosis infection in immunocompetent patients, serological tests confirm the presence of IgG antibodies. Similarly, our study tends to assume increased levels of IgG antibodies in immune-privileged entities that peak up to a plateau level then progressively decrease until negativation. In contrast, HIV patients IgG levels continually rise in instances of reactivation. That is to say, on the onset of infection IgM antibodies are produced as a consequent of active immunity, a process that lasts a week. These antibody levels continually increase between one and three months then decrease for the next nine months. Likewise, the production of IgG levels is stimulated two weeks after infection, which climaxes at three months and stagnates for the next six months. This prolonged stimulation of antibodies as a result of specific acquired immunity enhances a higher prevalence of morbidity as compared to that in the HIV infected patients. Moreover, the antigen binding avidity of IgG rises slowly in four months during toxoplasmosis acute infection (Basit, Nasir, Vohra and Shazlee, 2018). Nevertheless, the level of antibody production constantly drops after a period of a year due to a persistent latent cyst in immune-privileged organs like the brain and muscles. As such, the presented data in the graph shows a continuous increase of IgG levels up to its peak at 24 percent distribution frequency but later adjusts to a continuous decrease until 0 percent distribution frequency. Also, as the presence of high levels of IgG antibodies indicate an active immunity that protects the immunocompetent patient from any future reinfections (Kodym et al 2015). Evidently, the percentage difference graph indicates a significant difference in IgG levels of our test subjects. The graph compares the IgG levels of immunocompromised patients to immunocompetent subjects during toxoplasmosis infection. The demographics further contrast how the IgG levels of the two groups behave as the infection progresses. For instance, in the HIV patients the IgG levels continuously get a boost when the antigens are reactivated. However, the IgG levels of immunocompetent patients progressively decrease up to zero level in instances of reactivation as a consequence of adaptive immunity hence this study tends to accept the alternative hypothesis that there is a varied significance in the seroprevalence patterns in IgG levels of HIV patients and immunocompetent subjects. In this essence, immunocompetent individuals enduring the Toxoplasma gondii infection have a lower seroprevalence of IgG antibody levels as compared to immunocompromised individuals particularly in instance of the infection reactivation.

REFERENCES
- Basit, K. A., Nasir, S., Vohra, E., & Shazlee, M. K. (2018). Toxoplasmosis in an Immunocompetent Patient. Pakistan Journal of Medical Sciences, 34(6), 1579.
- Bharti, A. R., McCutchan, A., Deutsch, R., Smith, D. M., Ellis, R. J., Cherner, M., & Letendre, S. L. (2016). Latent toxoplasma infection and higher Toxoplasma gondii immunoglobulin G levels are associated with worse neurocognitive functioning in HIV-infected adults. Clinical Infectious Diseases, ciw655.
- Kodym, P., Malý, M., Beran, O., Jilich, D., Rozsypal, H., Machala, L., & Holub, M. (2015). Incidence, Immunological and Clinical Characteristics of Reactivation of Latent Toxoplasma gondii Infection in HIV-infected Patients. Epidemiology & Infection, 143(3), 600-607.
- Liu, Q., Wang, Z. D., Huang, S. Y., & Zhu, X. Q. (2015). Diagnosis of Toxoplasmosis and Typing of Toxoplasma gondii. Parasites & Vectors, 8(1), 292.
- Rougier, S., Montoya, J. G., & Peyron, F. (2017). Lifelong persistence of Toxoplasma cysts: A Questionable Dogma?. Trends in parasitology, 33(2), 93-101.
- Robert-Gangneux, F., & Belaz, S. (2016). Molecular diagnosis of toxoplasmosis in immunocompromised patients. Current Opinion in Infectious Diseases, 29(4), 330-339.
- Villard, O., Cimon, B., L’Ollivier, C., Fricker-Hidalgo, H., Godineau, N., Houze, S., & Candolfi, E. (2016). Serological diagnosis of Toxoplasma gondii infection: Recommendations from the French National Reference Center for Toxoplasmosis. Diagnostic Microbiology and Infectious Disease, 84(1), 22-33.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts