Developing a Community Health Profile
Introduction
The present assignment aims to develop the health profile of the community residing at the London Borough of Sutton, which is considered to be the largest borough in London. The profiling of the health of this particular community was considered to be important because of the varied types of population and environment of the place. The community health profile is measured with the help of two variables, i.e., demographic data and geographical information system. The clinical interventions that are related with regard to community health are primary, secondary and tertiary healthcare. The community health profile for this assignment is based on the available data on the long and short profiles and also the IOD deprivation profiles of Sutton obtained from Public Health England, 2019. At last the varied profiles such as social determinants of health, deprivation profile, status of wellbeing and the employment details of the study will be analysed using the Bradshaw taxonomy of health theories and based on the theories of population trends and transitions to effectively interpret the profile of the selected community. For those needing guidance on similar topics, seeking healthcare dissertation help can provide valuable insights. The data used for the analysis is currently sourced from PHE for the community of Sutton and the similar groups of figures were compared with the England to comprehend the overall health indicator statistics.
Background:
To define a community health profile, is an exhaustive gathering of data about a particular community. The information in a profile mirrors the health and wellbeing of the given community from a wide range of edges. The word “community” can be referred to a group of people residing at a particular area, a territory inside a province, a clan, or a multi-region locale (Ingram, 2012).
Characterising qualities of a health profile of a community involves the following:
Right of entry to quality training or education
The community people group normally mixes with the environment around them
Medicinal services and preventive wellbeing administrations
Right of entry to healthy nourishment
Openings for enhancing the physical strength and wellbeing opportunities (Ingram, 2012)
A needs appraisal of a community distinguishes the qualities and assets accessible within the network to address the issues of families, children and families. It offers detailed analysis of the indicators of health and well being which are described below at routine intervals and the figures are compared with average data of the England to analyse whether the trend is getting significantly better or worse with progressing time and what are the factors that needs to be addressed for betterment of the population. The evaluation centers on the abilities of the network, including its residents, offices, and associations. The health appraisal provides the recent information to the higher association thorough data about the present wellbeing status, requirements and health risks of the community. This data can help build up a network wellbeing improvement plan by supporting the strategies and the places where the assets should be distributed to give the optimum support to the community. The principle results of an evaluation of the requirements of a community are divided into 3 fundamental classes: Systems Change, Policy Change and Environmental Change (Ingram, 2012).
The term “monitoring” alludes to a constant, unique procedure of gathering information about wellbeing and varied maladies and their determinants in a populace over a characterized timeframe. Similarly the word “surveillance” is a more systematic type of information recording than checking (Baker, 2010).
The steps that are followed in the process of surveillance:
1. Detailing
2. Gathering of Information
3. Examination of Information
4. Evaluation and activity (Baker, 2010).
Continue your exploration of Community Health Promotion Initiative with our related content.
The need for monitoring and surveillance is very much crucial for the profiling of community health and requirements as this helps in the exploration of the potential warnings to health and also address the requirements for an effective model of health. According to the guidelines of the International Health Regulations (2005) every country need to keep up a complete detailing of the overall national response to public health surveillance and also should provide the detailed reports of the essential requirements that the nations want to accomplish to address the areas of concern. Systematic monitoring of the disease or infection threats should be confirmed based on the laboratory investigation and clinical monitoring and the number of cases affected or death cases gives a wide notion of the varied types of dangers to public health (Keller, 2009; WHO, 2008).
The Community Health Profile:
The successful compilation of the community health profile depends on the mass communication of the data from the professionals of public health to the common people with the aid of health marketing or one to one communication. Here the role played the social media is significant as it can create awareness of unhealthy habits and could effectively encourage people to endorse healthy life style for better health goal and the information available at the websites such as statistical data along with geographical information had helped many researchers to get a overall portray of the health of the community and in analysis. The community health profile of the based on the available data on the long and short profiles along with the deprivation profiles of Sutton obtained from Public Health England, 2019 (Korda, 2013).
The health indicators of the community are discussed in the following wide categories such as: demographics, deprivation, determinants and health status of well being.
Demographics:
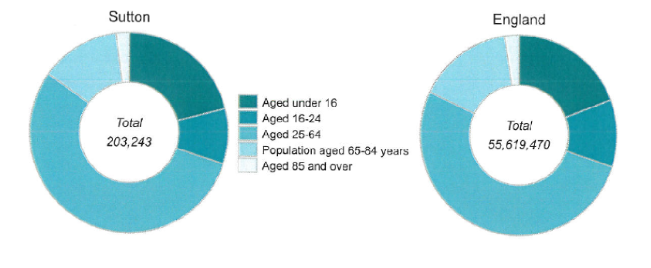
The demographics data is sorted based on gender and age range of the population:
The total population size of the Sutton is 203,243 as per the records of health profile whereas in comparison to the population size in England is 55,619,470 (ONS, 2017).
The population of individuals aged in between 0 to 15 years is 42777, whereas in England it is 10,638,000; in between 16 to 24 years in Sutton 18,138, whereas in England 6057,270; in between 25 to 64 years in Sutton – 111,471 population whereas in England it is 28,893,700; within 65 to 84 years in Sutton – 26,379 and in the England 8678,440. Ultimately the population size above 85 years and over in Sutton is 4478, whereas in England it is 1352,060 (ONS, 2017).

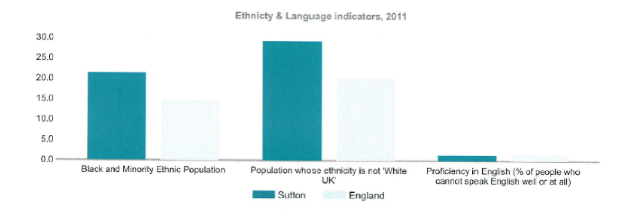
Ethnicity and Language:
As per reports from ONS, 2011 the data suggested that the black and ethnic minority population is 21.4% in the Sutton whereas in the England it is 14.6%; populace of non white ethnicity in Sutton – 29.1% whereas in the England it is 20.2%; populace who cannot talk in English language at all in Sutton – 1.4%, in the England – 1.7%.
The ethic black groups in the UK comprises of Bangladeshi, Pakistani, Black Caribbean people, East African and Asian people and Chinese. They usually suffer from various health inequalities and they suffer from disease such as cancer, cardiovascular diseases due to lack of education, financial poverty and unhealthy life styles (Norredam, 2011). The age and life style related disorders such as diabetes, stroke, obesity, smoking, hypertension, malignancies and premature mortality are commonly associated with the community as evident from the study of Benach, 2012. The nutrition related disorders such as obesity, malnutrition, cardiovascular issues, stroke, and type 2 diabetes are also common among the studied community (Norredam, 2011).
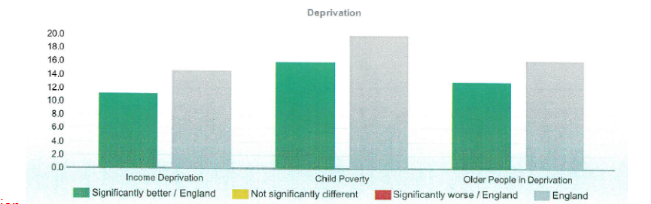
Deprivation:
As per the indices of deprivation score IMD for Sutton is 14.6 whereas for the England – 21.8. When the percentage data was analysed it was observed that Income Deprivation (%) in Sutton is 11.1, in England – 14.6; Child Poverty (%) in Sutton is 15.9 whereas in the England it is 19.9; Elderly adults (above 60 years) in deprived condition in Sutton is 12.9 and in the England it is 16.2 (PHE, UTLA, 2013). The percentage figures with regard to income deprivation for the Sutton are significantly better when compared with the England, similar trends were observed for both the profiles of child poverty and elderly adults living in deprived condition.
Social Determinants of Health:
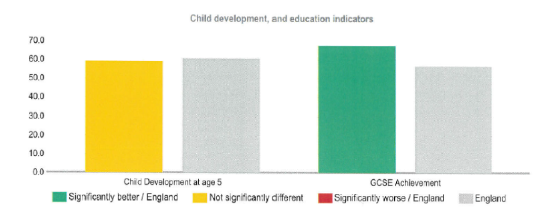
Child Development and Education
As per the study report of Sutton (PHE, UTLA, 2013) the outcomes on child development and education highlighted that -Development of child at the age of 5 years in Sutton is 1578 (59.1%) whereas in case of the England – 387,000 (60.4%); Accomplishing 5A star to C in GCSE of 2013 -14 in Sutton is 1482 (67.4%) whereas in the England it is 315,795 (56.6%).
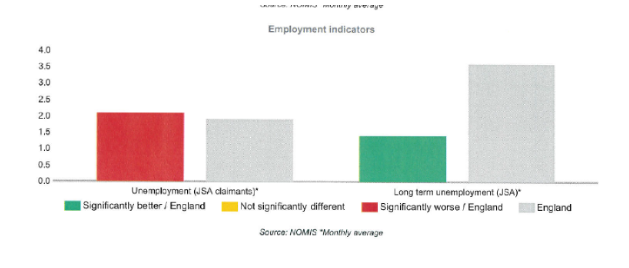
Employment Details:
Again according to the source of UTLA, 2013 the employment indicators of 2017 -18 highlighted that the job seekers in Sutton (2727; 2.1%) whereas in the England it is 665,871 (1.9%) which is rate/ 1000 working age populations. Similarly the job seekers for more than one year it is 180 in Sutton and 124,616 in the England.
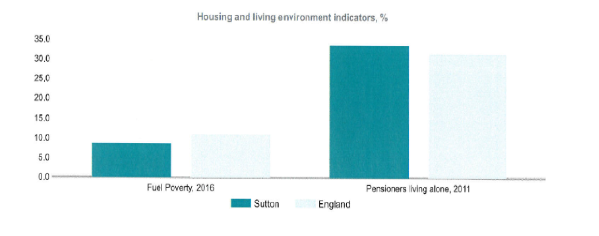
With respect to the housing and environment of living indicators, the ONS census, 2011 reported that the fuel poverty in the year, 2016 in Sutton is 7051 whereas in the England it is 2550,270. The pensioners who are residing alone in Sutton in the year, 2011 were 9203 whereas in the England it was 2,725,600.
Status of Well being:
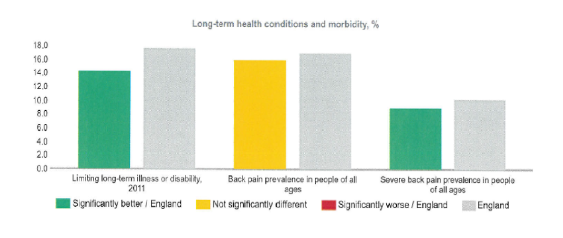
Long term health and Morbidity Analysis:
According to the source of ONS, 2011 and PHE the predominance of long term morbidity and disability in Sutton was 27,189 whereas in the England it was 93,52,590. The data percentage of predominance of back pain among the populace of all age groups Sutton was 16% and in the England it is 16.9%. Similarly the predominance of severe back pain among all ages was 9% in Sutton and 10.2% in the England.
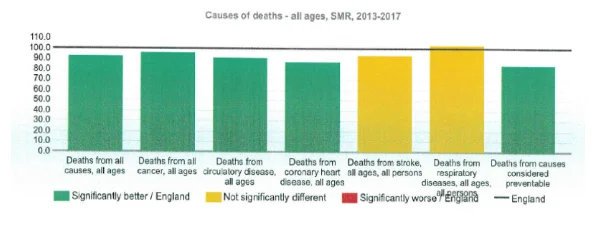
As per the data of ONS, 2018 the reasons and numbers of premature mortality are:
The Standard Mortality Ratios (SMR) due to varied reasons below age of 75 years in the Sutton is 87.7 whereas in the England it is 100; mortality as a result of all forms of malignancies in Sutton is 93 whereas in case of the England it is 100. Moreover, mortality as a result of circulatory diseases in Sutton is 85.6 whereas in case of England it is 100 (ONS, 2018).
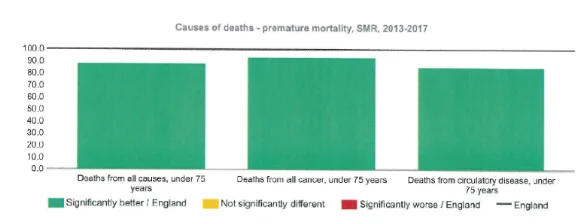
The analysis of all causes of mortality in Sutton is 92.6 whereas in England it is 100 which include malignancies, coronary artery diseases, stroke and respiratory diseases (ONS, 2018). Therefore the data suggest all the parameters are significantly better when compared with the England.
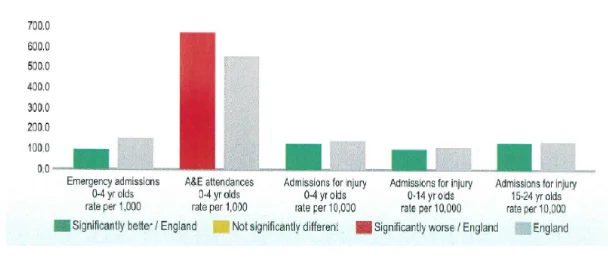
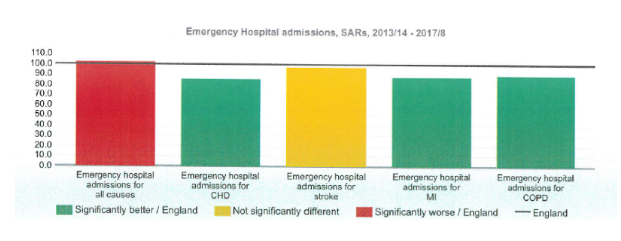
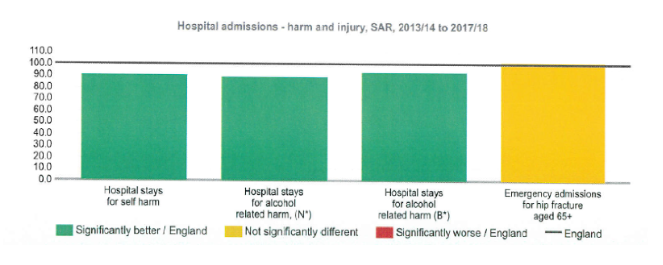
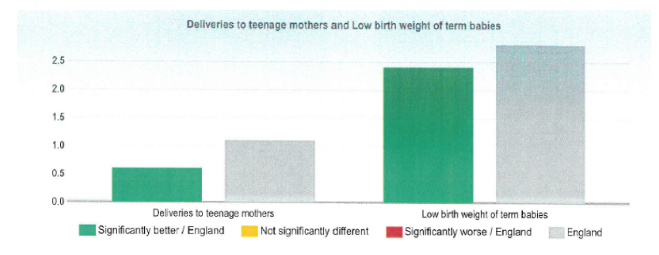
Hospital Admissions Data Analysis:
The hospital admissions rate is expressed in terms of Crude rate/1000 (NHS Digital, 2018)
The data on maternity and child health as per the source of Hospital Episode Statistics, NHS digital and ONS data rate of delivery of teenage mothers, crude rate of fertility and term babies of low birth weight highlighted that the figures are significantly better than England (NHS Digital, 2018).
Life Expectancy At Birth:
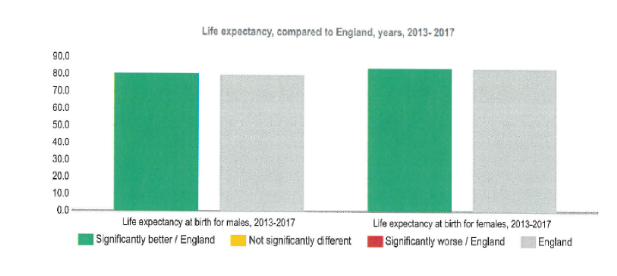
The data of Sutton is comparatively than England for both the genders (ONS, 2018).
Healthy Life expectancy:
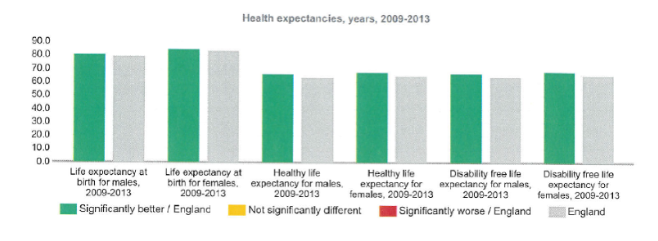
The overall figure analysis shows that the health life expectancies and the disability free expectancies are better than England (ONS, 2018).
Analysis of Behavioural Risk Factors:
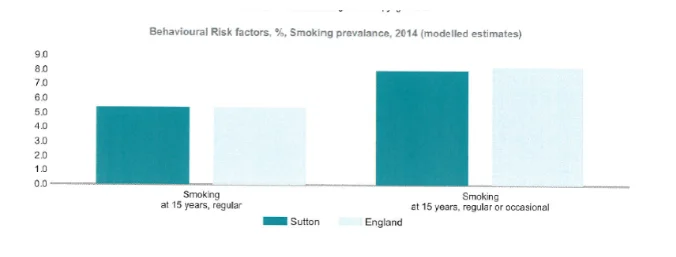
The numbers are comparable for Sutton with respect to occasional and regular smokers (PHE, 2018).
Implications of the Findings:
As per the demographics data the total population size of Sutton was significantly small in comparison to England and the ratio of male to female was found to be comparable according to the figures 1 & 2. The socioeconomic status is considered to be a basic cause of health diseases (Flaskerud, 2012). The data on overall deprivation also demonstrated that Sutton is significantly better in all terms than England. It is evident from past studies that people who belong to lower economic status suffers from expanded rate of mortality along with age wise mortality due to improper diet, lack of physical activities and habits of smoking and drinking (Flaskerud, 2012). However, the data on hospital admissions due to CHD, MI, stroke were marginally better than England which can be attributed to the improper life styles of people and habits of smoking and alcohol related harm were also comparable to England though little better. Coronary illness is the most regular condition in more seasoned grown-ups and the significant cause for death. Failure of heart, disease of coronary artery, and atrial fibrillation are normal purposes behind hospital visits and stays. Ordinary maturing causes your heart and veins to harden, which can prompt these conditions in later years. For individuals more aged than 75, hypertension is the most widely recognised heart condition (Albus, 2010). The rate behavioural disorders and self destruction was marginally high among the population of Sutton highlighting about the unhealthy habits of life due to lesser number of employment, lack of education and up taking of bad habits or wrongdoing though the education rate was found to be comparatively high than England (Walsh, 2011). The health awareness and screening of diseases should be increased as mortality rate due to CHD, malignancies, circulatory and respiratory diseases can be lowered down though it is significantly much better than England.
Bradshaw’s (1972) taxonomy of need formulated a framework to make a 'genuine' need comprehendible. His proposition was to initially outline four kinds of social needs, in particular, (a) normative; (b) felt; (c) expressed; and (d) comparative, at that point to inspect their quality in a given situation (Bradshaw, 2013). Through the Bradshaw’s need theory the varied needs such as normative which includes the health screening for malignancies, awareness about rising CHD, diabetes and respiratory disorders and the significance of life formative changes has to be met. Through awareness and enhancement of employment the expressed need will be augmented and people will visit physicians for health check up for early detection and cure of disease. The comparative need might demand about the well established health care services as the populace of England receives. The asset based community development strategy (ABCD) is a systematic methodology utilized for the sustainable development of a community based on the potentialities and limitations of the community. The process involves the accessing the need of the resources, skills and experiences available within a community and formulating the strategies in such a manner which will allow the members to take up the appropriate action. By using these skills of the individuals within the community they might be able to develop at home or at work such as hair cutting, carpentry, wallpapering, baby sitting, etc. It utilizes the asset mapping strategy and this will eradicate the poverty and unemployment to a certain extent and will have positive impact upon health (Misener, 2016). As per demographic transition model the populace of Sutton has higher birth rate or crude fertility rate and the death rates of infants are also lower in comparison to England (Lesthaeghe, 2010). However, the education rate was also found to be higher but the employment rate is lower leading to high violence rate and obese adults. Therefore, to increase the health status the level of employment, medical facilities and health awareness has to be increased. When the data is analysed based on epidemiological transition all the parameters such as age, life expectancies, fertility rate all has accomplished significantly better level with lower mortality rate (Defo, 2014). The data on communicable diseases such as tuberculosis (TB) and sexually transmitted disease (STD) found to be contradictory when compared with the England demonstrating 780.2 for STD in local area whereas in the England it is 850.6, and for TB it is 10.5 for Sutton whereas 9.19 for the England. Therefore, the incidence of TB is marginally high for Sutton; high rate of communicable diseases highlighted about the lack of hygiene among those people (Sahoo, 2015). For the non communicable disease which falls under the category of long term health conditions and morbidity, the outcomes highlighted that any kind of long term disability or back pain is significantly lower than the England populace. Figures on obese children also highlighted towards the ignorance and lack of education about healthy lifestyle among the parents (Sahoo, 2015). However, the nutrition transition model highlighted about unhealthy nourishment propensities and unhealthy life styles among the populace due to which CHD, MI, diabetes, obesity and stroke getting worsened with progress of time. These aspects have to be addressed for better health profile of the community (Shetty, 2013).

Conclusion
The community of Sutton is significantly better in overall terms when compared to England however, the employment level is comparatively low and the health risk of certain life style disorders are increasing. Therefore, it is suggested that the awareness of health along with medical facilities has to be introduced within the community populace and the skills of the community can be utilised to create employment for the populace to meet their needs which would in turn lower down the violence or crime rate and improve their health conditions. When the health indicator values are compared with the England population no need was felt for the population of Sutton that demands immediate attention.
Continue your journey with our comprehensive guide to Detention Criteria Under the Mental Health Act of 1983.
References
- Ingram, M., Reinschmidt, K.M., Schachter, K.A., Davidson, C.L., Sabo, S.J., De Zapien, J.G. and Carvajal, S.C., 2012. Establishing a professional profile of community health workers: results from a national study of roles, activities and training. Journal of community health, 37(2), pp.529-537.
- Baker, M.C., Mathieu, E., Fleming, F.M., Deming, M., King, J.D., Garba, A., Koroma, J.B., Bockarie, M., Kabore, A., Sankara, D.P. and Molyneux, D.H., 2010. Mapping, monitoring, and surveillance of neglected tropical diseases: towards a policy framework. The Lancet, 375(9710), pp.231-238.
- Keller, M., Blench, M., Tolentino, H., Freifeld, C.C., Mandl, K.D., Mawudeku, A., Eysenbach, G. and Brownstein, J.S., 2009. Use of unstructured event-based reports for global infectious disease surveillance. Emerging infectious diseases, 15(5), p.689.
- World Health Organization, 2008. International health regulations (2005). World Health Organization.
- Korda, H. and Itani, Z., 2013. Harnessing social media for health promotion and behavior change. Health promotion practice, 14(1), pp.15-23.
- England, N.H.S., 2018. NHS digital. Hospital accident and emergency activity.
- Walsh, R., 2011. Lifestyle and mental health. American Psychologist, 66(7), p.579.
- Albus, C., 2010. Psychological and social factors in coronary heart disease. Annals of medicine, 42(7), pp.487-494.
- Sahoo, K., Sahoo, B., Choudhury, A.K., Sofi, N.Y., Kumar, R. and Bhadoria, A.S., 2015. Childhood obesity: causes and consequences. Journal of family medicine and primary care, 4(2), p.187.
- Benach, J., Puig-Barrachina, V., Vives, A., Tarafa, G. and Muntaner, C., 2012. The challenge of monitoring employment-related health inequalities. J Epidemiol Community Health, 66(12), pp.1085-1087.
- Norredam, M., Kastrup, M. and Helweg-Larsen, K., 2011. Register-based studies on migration, ethnicity, and health. Scandinavian journal of public health, 39(7_suppl), pp.201-205.
- Bradshaw, J.R., 2013. Jonathan Bradshaw on social policy: Selected writings 1972-2011. University of York.
- Misener, L. and Schulenkorf, N., 2016. Rethinking the social value of sport events through an asset-based community development (ABCD) perspective. Journal of Sport Management, 30(3), pp.329-340.
- Flaskerud, J.H., DeLilly, C.R. and Flaskerud, J.H., 2012. Social determinants of health status. Issues in mental health nursing, 33(7), pp.494-497.
- Lesthaeghe, R., 2010. The unfolding story of the second demographic transition. Population and development review, 36(2), pp.211-251.
- Defo, B.K., 2014. Demographic, epidemiological, and health transitions: are they relevant to population health patterns in Africa?. Global health action, 7(1), p.22443.
- Shetty, P., 2013. Nutrition transition and its health outcomes. The Indian Journal of Pediatrics, 80(1), pp.21-27.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts