Maximum Oxygen Uptake Test on Female Recreational Cyclist
INTRODUCTION
According to Poole et al. (2008), the maximum oxygen uptake (VO2max) is the maximum amount of oxygen (O2) that can be used while performing intense exercise. It is the individual’s maximum capacity of the pulmonary, cardiovascular as well as muscle systems to uptake, transport and use of O2 while. There are a few determinants of VO2max: arterial and venous O2 saturation, circulation rate as well as O2 capacity of the blood (Hill et al., 1924). There are a few criteria in determining the ventilation cut-off point including “an increase in the respiratory exchange ratio (RER), a nonlinear increase in ventilation, a nonlinear increase in carbon dioxide (CO2) production, an increase in end-tidal O2 partial pressure, the beginning of a systematic increase in the ventilatory equivalent for oxygen (VE/VO2) without an increase in the ventilatory equivalent for CO2 (VE/VCO2)” (Myers & Ashley, 1997, p.790). VO2max can be affected by many factors such as cardiac output (CO), the functioning of peripheral circulation (O2 tissue extraction), working capacity and efficiency of heart, lungs and blood vessels, O2 diffusion capacity as well as metabolism capacity in skeletal muscles (Bassett & Howley, 1997). For those engaged in research or academic work related to this topic, healthcare dissertation help can provide essential support and resources.

The direct VO2max measurement is a reliable and validated method of assessing cardiorespiratory fitness (Grant et al., 1995). However, this method is time-consuming and expensive thus methods of prediction are commonly used as a cheaper and faster alternative. The O2 uptake is measured using the treadmill or cycle ergometer when the work rate gradually increases to the subject’s exhaustion or O2 plateau, point of achieving maximum HR and CO as well as VO2max (Spurway, 1992). As the work rate increases, the O2 uptake also increases to the point when the individual achieves VO2max and no further increases in O2 uptake is seen even though there is a continuous work rate increase (Astrand, 1960). However, in many cases, the subjects will become fatigued before reaching their O2 uptake plateau thus it is often difficult to determine if VO2max was achieved (Bassett & Howley, 2000). These findings showed a need to determine other VO2max criteria such as respiratory exchange ratio (RER: the ratio of expired carbon dioxide (VCO2) to oxygen (VO2) consumed), maximum HR (+/- 10bpm) as well as the concentration of blood lactate (8-10mmol/l) (Poole et al., 2008). However, the maximum incremental test can determine VO2max, gas exchange threshold, O2 uptake as well as work efficiency, four aerobic parameters, in one, short test rather than long, discontinuous trials (Whipp et al., 1981).
The VO2max test allows researchers to gain a more in-depth view of the participant’s fitness level. In this work, VO2max of a 35-years-old recreational cyclist will be measured and analysed during cycle ergometer test. The participant is preparing for two cycling competitions: summer one in Spain and autumn event in Poland thus advice on performance improvements in general as well as heat training will be provided. The protocol was specifically designed for cycling athlete and appropriate for her training status and program.
METHODS
A 35-years-old, female, healthy recreational cyclist participated in VO2max test on 18.11.2019 at 10.30 at Edinburgh Napier University Laboratory. Before the experiment, the subject was asked to complete a pre-activity readiness questionnaire to screen for any underlying health conditions and contraindication of the participation in the study, none were detected. The informed consent was obtained from the participant and she was informed about her right to withdraw from the experiment at any time without giving any reason. Participant’s anthropometric information and blood pressure (BP, using the Blood Pressure Unit, Novacor Diasys Integra System UK) were taken (Table 1). The BP higher than 140/90mmHg would exempt participant from the study.

Testing Protocol
The participant was given a detailed explanation of the nature and protocol of the experiment and was informed that she is expected to give 100% effort and work on her maximum potential level. The participant was asked to cycle on the cycle ergometer (Velotron Pro,USA), starting with 5min of warm-up, with a firmly fitted breathing mask covering nasal and oral passages until her HR reaches its maximum (220 – 35 (age) = 185bpm +/- 10bpm). On the other side, breathing mask was attached to a CPX machine (Jaeger CPX, Germany) allowing constant monitoring of the participant’s VO2. HR monitor (Polar FS1 Heart Rate Monitor, Finland) was fitted to the subjects’ chest allowing constant monitoring of HR throughout the test by checking the readings on a watch. During the test, the assigned person kept track of time using a stopwatch to ensure accurate recording. The participant started on initial work rate (WR) of 60W. At 2-minute intervals, based on the workload guidelines for an aerobic fitness test, the WR was increased by 25W, HR and VO2 were recorded and the participant was asked to point a number on the Rating of Perceived Exertion (RPE) scale to check the participant’s feeling about the test. The experiment continued until the subject’s exhaustion after which the last reading was recorded, and cool down time implemented. It is a maximum test thus the subject was expected to give her maximum effort during the experiment.
All information of pre and post VO2max test were entered in Excel document. The CPX machine allowed to analyse O2, CO2 and volume necessary to calculate VO2, VCO2 and VE and assess participant’s VO2max.
RESULTS
The following section presents the main findings of the study further discussed in the Discussion section.
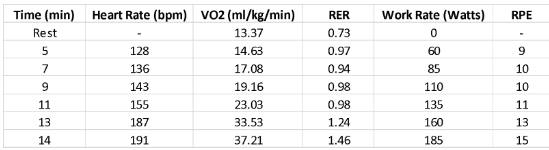
As the test time and WR increases (from 60 to 185W), the HR, O2 uptake and RER also increase. The body slowly becomes fatigued which is represented by the increase in RPE score (from 9 to 15). It can be also assumed that participant used her maximum effort as the final HR (191bpm) at around 14min into the test and WR=185W is at subject’s maximum.
Participant’s RER value starts with 0.73 at rest suggesting carbohydrates (CHO) as a main source of energy and as the exercise begins, it increases but stays below 1 until 11min into the test when the WR is on 135W and the HR reaches 155bpm. However, just after reaching 11min into the test at WR 160W the body switch entirely to CHO as the RER value becomes 1 and above.

Table 3 shows that participant’s absolute VO2max is 41 at the intensity of cycling 185W, which according to norm values for VO2max is above average for a 35-year-old female. The two Ventilatory thresholds are also determined: VT1=19ml/min/kg and VT2=37ml/min/kg. Participant reached her VO2 peak (38ml/min/kg) but not her VO2max.

CPX machine gas analysis allowed to plot the VCO2 against VO2 which helped to identify the LT (the point when VCO2 increases away from VO2 so the relationship is no longer linear) at about 32ml/kg/min and 160W (Table 2).
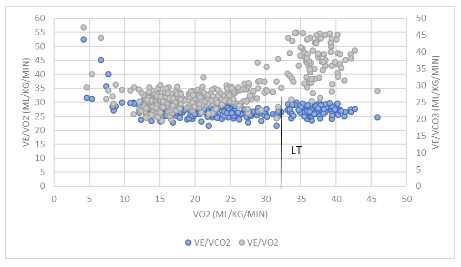
The estimated LT, the point where VE/VO2 increases away from VO2 and there is no matching increase in VE/VCO2 is around 30ml/min/kg and is reached at exercise intensity 160W (Table 2). After this point, the VE/VCO2 and VE/VO2 divert from each other.
DISCUSSION
In order to obtain reliable and valid results, the direct measurement of VO2max was conducted by gas analysis with the use of CPX machine. As the test time and WR increases, the HR, O2 uptake, RER and RPE also increase. This is in line with Hill and colleagues work (1924) showing that as the WR and HR increase, the O2 uptake also rises. The results noted in Table 2 show that O2 uptake increases from 14.63 ml/kg/min to 37.21 ml/kg/min as the WR of cycling increases. The body works harder, the HR rises, and muscles need more energy thus there is an increase in O2 uptake as a respond for the increased demand of the body for the O2 and removal of CO2. The subjective exertion and response to exercise intensity were regularly assessed using RPE, the scale developed by Borg in 1982. The RPE combines feedback of cardiorespiratory, metabolic and thermal stimuli and is moderated by psychological aspects such as cognition, previous experience, understanding of the task (Branco et al. 2013). The scale ranges from 6, at rest, to 20, at the maximum effort which corresponds to HR of 60-200bpm. The RPE increased with the exercise intensity due to participant slowly becoming fatigued. At the last reading, at around 14min, the HR was 191bpm, higher than predicted maximum HR and the RPE was scored by the subject at 15 which indicates that participant perceived the test as hard and used her maximum effort
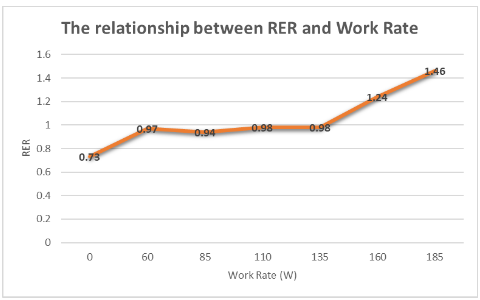
RER is the ratio of CO2 production (VCO2) and O2 consumption (VO2) and it allows to interpret the utilization of macronutrients, CHO or fat, as the primary fuel source during exercising (Figure 1). From Figure 2, it is seen that when at rest, the participant uses mostly fats as the main source of energy (RER=0.73). As the WR increases, there is a higher demand on respiration to remove the excess of CO2 and provide the body with enough energy derived mostly from the CHO as this is a quicker process since one glucose molecule needs less O2 to break down compared to a fat molecule. In this case, fats are not able to provide enough energy to the body at the needed rate. Participant’s RER value stays below 1 until 11min into the test when the WR is at 135W and the HR reaches 155bpm. This suggests that until this point, the body was mainly using a mixture of fat and CHO as a source of energy as predicted during low-intensity, steady exercise. RER increases up to 1.56 at WR=160W suggesting the switch from fat to CHO as a main source of energy.
The LT is the exercise intensity at which there is a significant and rapid increase in blood lactate concentration, there is higher lactate accumulation than removal (Bishop et al., 2000). This increase in lactate accumulation can lead to metabolic acidosis, abnormal muscle contraction, higher ventilation rate and O2 kinetic change (Myers & Ashley, 1997). Endurance training is seen to improve performance by increasing mitochondria number and their enzyme activity which can increase fat oxidation and decrease lactic acid accumulation (Bassett & Howley, 2000). Bang (1936) showed in his work that as the exercise intensity increases, the lactate concentration, ventilation rate and O2 consumption also increase. Beaver and colleagues (1986) determine bicarbonate as the body’s main acids buffer thus increase in CO2 production can be observed when there is blood lactic acid rise. In this experiment, the non-invasive method, analysing gas samples, was used to determine LT as it was cheaper and quicker than analysing the blood samples. The gas analysis identified the LT at about 32ml/kg/min (Figure 2) and 30ml/kg/min (Figure 3) by looking at the relationships between VO2, VCO2, VE/VO2 and VE/VCO2. In addition, ratios of VE/VCO2 and VE/VO2 rise more drastically after the lactate threshold (Figure 3; Spurway, 1992). Looking at the relationship between VCO2 and VO2 (Figure 2), the point where the slope change can be observed determines the point at which there is a surplus of CO2 in the body (anaerobic threshold) and gas levels change in the bloodstream (Beaver et al., 1986). At the anaerobic threshold when there is most of the energy provided by anaerobic metabolism, increase in lactic acid in the bloodstream is observed causing rise in ventilation rate to remove an excess of CO2 and lowering the acidity of the blood. At this threshold, the VE/VO2 ratio increases as there is higher pulmonary ventilation than O2 uptake (Figure 3). There are two ventilatory thresholds identified and presented in Table 3. The first one (VT1) indicates the point where there is an increase in breathing rate and lactate in the blood as the exercise intensity increases. After reaching VT1, the participant is no longer able to talk comfortably but the exercise can continue for a long time (30-90min) at this WR. The second ventilatory threshold (VT2) is a point of a further increase in breathing rate and rapid build-up of blood lactate and participant is no longer able to talk. The exercise is less likely to continue for longer than 60-120s. The increase in this threshold is the indicator of performance improvement.
Endurance training increases stroke volume and ventricles capacity to fill up with the blood due to increased heart size, wall thickness and better stretching capabilities. This together with decreased peripheral resistance due to increased blood vessels vasodilation allow for the more forceful contraction (McArdle et al., 2000). Blood supply to skeletal muscles is at about 20% during rest but it increases significantly during exercising up to 80% of CO as there is an increased demand for the O2 and nutrients in the muscles thus blood flow must be primarily directed there (Wilmore & Costill, 2005). Gledhill et al. showed that increase red blood cells number and as a result haemoglobin concentration following endurance training, increases participants’ VO2max by about 5 to 10%. As the O2 carrying capacity increases, the VO2max also increases in athletes, but no change was observed in untrained individuals (Kravitz & Dalleck, 2000). Bassett and Howley (2000) also showed that higher levels of mitochondrial enzymes can also improve exercise performance and increase VO2max since more mitochondria allow more efficient O2 extraction from the bloodstream to the muscles. The muscles metabolism is also improved due to the presence of oxidative enzymes responsible for CHO and fats breakdown to provide energy. Some of the other effects of long-term exercise training include lower resting HR improving recovery time after exercise, a higher number of capillaries in skeletal muscles, the volume of blood and red blood cells count, lower risk of heart diseases.
Esfarjani and Laursen (2007) study found that that a 10-week high-intensity interval training significantly improved VO2max and LT in the participants increasing their aerobic capacity. This shows that a combination of different training types, with correct frequency and duration, could promote better performance in participants. Wenger and Bell (1986) demonstrated that endurance running of 35min at or just above threshold, three times per week alongside with two interval sessions lasting 15min increased participants’ performance, increasing their VO2max by 6.4% over eight weeks. It was approved that integrating two sport-specific strength training sessions alongside an endurance training programme would provide a more significant performance increase (Karsten et al., 2016). Another good training method is to exercise at threshold training (maximum aerobic stable phase) which is a person’s optimal WR for endurance performance. Training at a higher intensity may lead to relying on anaerobic metabolism and this, in turn, could cause built-up of lactate, fatigue, muscles shut down and, at later stages, muscle damage and decreased aerobic capacity. Training at lower intensity could prevent an athlete from maximal benefit to aerobic capacity. Some researchers suggest that RPE scale is an accurate and reliable method of determining exercise intensity as it is related to the lactate fluctuation during exercise (Weltman, 1995). It was shown that value of 13-15, “somewhat hard” and “hard”, on RPE scale indicates reaching the LT (Weltman 1995). In this experiment, participant’s LT based on RPE scale would be determined at WR about 160W (Table 2). The LT determines the highest exercise intensity that athlete can sustain for a long time. If this point is determined, the trained athlete can cycle at this speed for a very long time, even for hours but LT differs between individuals thus there is a need to design exercise plans for athletes based on their conditioning profiles.
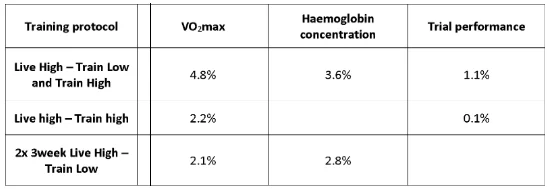
Many training recommendations could be given to the athlete cyclist. One of them is altitude training (AT) which shows promising results in increasing VO2max, exercise capacity and endurance performance. The “Live High – Train Low” (LHTL) training protocol is most often used as it was proven to allow acclimation of the body to lower level of O2 available at altitude but then train with maximum efforts and compete in lower altitudes (1200m or below) as the muscles have a maximal O2 availability for aerobic performance and can work much harder (Chapman, 2016). It includes living at 2200-2500m and training at high intensity at 1300m or below, for 4 weeks. Living at high altitude makes the athletes adapt to breathing thinner air which in turn improve exercise performance at sea level. During the acclimation to a higher altitude, athletes gain more red blood cells increasing their O2 carrying capacity. When they come back to the sea level to compete, their muscles receive an extra boost as there is more O2 available. This can improve ventilatory response, muscle buffering capacity and increase erythropoiesis leading to better performance by a few per cent which sometimes can be crucial in a competition (Chapman, 2016). It was shown in the study by Chapman et al. (1998) that 54% of elite athletes showed performance improvements following LHTL training after returning to sea level. They also supported more beneficial LHTL protocol over traditional live high – train high (LHTH) training as only 23% of participants in this group reported performance improvement. Moreover, Bonetti and Hopkins (2009) showed in their study that performance improvements were only seen following LHTL (4%) comparing to LHTH (1.6%) or live low – train high (0.6%). However, recent studies showed that a mix of different altitude training protocols provides even better results. Robertson et al. (2010) showed that the combination of LHTH and LHTH increases VO2max and haemoglobin mass to a higher extent comparing to 3-week LHTL or LHTH alone (Table 4). This combined training protocol improves greatly cycling performance (Garvican et al., 2011).
Most of the AT takes time to give desirable results. Researchers determined the optimum altitude of 2000-2500m for 4 weeks to increase the erythropoiesis and VO2max and reported that these benefits last for about 2-3 weeks after returning to sea level (Gore et al., 1997; Baumann et al., 1994; Wilber, 2001). Often, the athletes cannot take part in AT camps, thus forms of altitude stimulation were discovered such as nitrogen houses or hypoxic tents. Furthermore, there is a lower appetite observed in athletes at altitude increases the risk of not providing the body with enough CHO and fats and starting to utilize proteins as a source of energy leading to loss of muscle mass. Thus, it is important for the athletes doing AT to take extra vitamins to lower oxidative stress and drink extra fluids to prevent excessive diuresis and dehydration. Schmidt (2002) proved that prolonged exposure to altitude increases haemoglobin concentration, erythropoiesis, ventilation rate, O2 transport, blood viscosity, capillary density and as a result increases O2 carrying capacity and aerobic power when back to the sea level allowing athletes to train harder and compete better. He also determined other biological improvements in muscle energy efficiency such as increased oxidative enzyme activity, mitochondria number, fatty acids utilization, muscle buffering, lactic acid tolerance and improved glucose transport.
Exercising in hot environment adds physiological pressure on the working body including increased body temperature, pressure on the cardiovascular system and changed metabolism. This can lead to thermal distress, reduced aerobic performance as well as a higher risk of heat illness (Nybo et al., 2014; Sawka et al., 2011). In order to avoid this, it is important to go through the heat acclimation (HA) stage that would improve exercise capacity. Roberts and colleagues (1977) and Nieman (2011) showed that previous heat exposure and acclimatization have significantly improved athletes’ thermoregulation, metabolism, working of cardiovascular system, fluid and electrolyte balance. During HA the person exercise in heat repeatedly and this heat exposure is enough to cause increased sweating rate and body temperature. Sawka et al. (1996) stated that healthy people can exercise efficiently in heat conditions following proper heat adaptation training, fluid and nutrient intake and access to shade. Athletes with higher aerobic fitness induce HA much quicker and its benefits last longer (Armstrong & Pandolf, 1988; Pandolf, 1998).
There are many physiological effects of HA to improve endurance performance allowing an individual to exercise in the conditions that used to be too hard to succeed. These benefits include increased blood flow to working heart, skeletal muscles as well as to skin, improved thermoregulation and sweating rate, cardiovascular and vasomotor responses, better and more efficient fluid balance, lower body dependence on glycogen for energy supply and lower lactate accumulation (Périard et al., 2015; Sawka et al., 1996, 2011; Gonzalez & Gagge, 1976; Lorenzo et al., 2010; Nielsen et al., 1993; Racinais et al., 2015; Taylor, 2014). The earlier onset of sweating improves body cooling by reducing skin temperature and heat accumulation and storage and this, in turn, will lower cutaneous blood flow and change blood distribution to central rather than peripheral circulation (Sawka et al., 2011). There is proper nutrient supply to the working muscles and waste products removal as there is more blood diverted to muscles but also to the skin for evaporation and cooling process. Moreover, the person training in a hot environment without previous acclimatization can loose with sweat high amount of sodium (Sawka et al., 1996). Following HA, sodium is kept in sweat glands and a much lower amount of this nutrient is secreted with sweat. This sodium retention leads to total body water content increase (Mack & Nadel, 1996). Thus, the right supplementation and hydration need to be made during training and competing to replace lost fluids. In addition, athletes reported decrease perceived effort, better thermal comfort and higher thirst drive following heat acclimation. Exposure to heat for a long time determined the need for more efficient sweat response including sooner sweating onset (lowering core temperature), higher sweat rate (evaporative cooling), increasing evaporation surface area, sweat composition change (retaining minerals), plasma volume rise (heat transfer capacity improvement).
Exercise in the heat is the most often used method of training for HA and is dependent on the exercise intensity, time, frequency and heat exposure number (Périard et al., 2015; Sawka et al., 2003; Taylor, 2014). Heat acclimatization and acclimation, are shown to improve athletes’ heat adaptation and endurance performance. Heat acclimatisation is a passive heat exposure in natural climate for 1-2 weeks. Heat acclimation (HA) is an active training protocol in which person trains in a hot, controlled environment. There are two main HA protocols. Active protocols include exercising in hot conditions. This protocol includes submaximal exercising in environmental, heat chamber for 60-120 min a day for 10-14 consecutive days, which allow close control of the conditions such as humidity, temperature, O2 level. It is the best way of heat training because it is possible to set desired conditions that replicate the environmental conditions of the event destination, but it is very expensive and the access to heat chambers is limited. If there is no access to such complex and expensive equipment/labs, exercising with extra clothes in the DIY chamber, hot room, at home can be also used. The heat generated by the working muscles and the heat added from the central heating would increase the body core temperature causing sweating, the main HA stimuli. The passive protocols are seen as less effective in HA, but they are less time-consuming, easier to follow and do not diminish other training programs. This includes hot water bathing straight after the cycling exercise when the body core temperature is still increased. Zurawlew et al. (2016) determined 5% performance time improvement following that 40min hot bath in 40°C water for a week. Another strategy is to use Hyperthermic conditioning using an artificial source of heat such as a sauna. The protocol includes exercising for about 60min before using sauna, for 15min on at least 3 occasions per week. During this training, body works harder and is challenged to meet energy requirements leading to efficient and strong heat adaptation. In the study by Scoon et al. (2007), it was proven that a dozen of post-exercise sauna exposures, HA, in 3 weeks improved time to exhaustion in cooler conditions and performance in athletes.
The best HA protocols include interval training and recovery activities in cooler times of the day, for example in the morning and moderate-intensity endurance exercise conducted during the hottest parts of the day. It is also important to start HA at least 2 weeks before travelling to a hot environment and terminating the heat training at least a week before the event to make sure any negative effects of heat would have time to ease. The traditional HA protocol is based on a repeated exercise in heat at the same exercise intensity, but this was proven to not cause a full-body adaptation to the heat. The controlled hyperthermia, exercise workload where there is a progressive overload used is more likely to cause a full HA and further body adaptations (Taylor, 2014; Périard et al., 2015). The heat stress, exercise WR as well as duration may need to be gradually increased. It is important to add that well-trained athletes are fitter and may need to use higher exercise intensities. About 1-2 weeks of aerobic training in the heat, 90-120mins per day, was determined as the optimal time for allowing HA with benefits lasting up to 10 days (Pandolf, 1998; Sawka et al., 1996; Eichna et al., 1950). When the person is exposed to heat again, the acclimatization takes less time (Weller et al., 2007). The study done by Racinais et al., (2015) found that cyclists’ performance was 11min slower when cycling 43km in the hot conditions (37°C) comparing to the cooler environment (8°C) but after a week of HA this difference was lowered to 3min and after 2 weeks the performance times in hot and cold conditions were the same. Moreover, Lorenzo and colleagues (2010) conducted HA on 12 sub-elite cyclists who were asked to perform 90min of moderate-intensity cycling exercise each day for 10 consecutive days in 40°C and humidity at 30%. They stated that significant performance in heat improvement was observed following heat acclimation training including a 5% increase in athletes’ VO2max and lactate threshold.
There are few important pieces of advice given to the participant that would help her in her competition training retrieved from the work of Day by Day Coaching (2015), Smyth K. (nd) and Carmichael Training Systems (nd). It is important to properly hydrate during heat training and competition to provide the body with sufficient water and electrolyte to prevent a rise in core temperature which can happen when the person becomes dehydrated. During training or competing in heat, the body loses much more fluids and if this loss is over 2% of body weight, the endurance performance and motor skills can be reduced, fatigued increased and lower motivation as well as primary stages of heat illness observed. During the event, it should be remembered to find a balance between wearing the lightest and breathable clothes but also covering the body from the sun. Sun cream must be regularly and plentifully applied to protect the cyclists from skin burns that can lead to an increase in core temperature and overheating. Good idea is to drink frozen slushy drinks as they are successful in maintaining a lower core temperature. The participant was advised to make them on her own by blending ice with electrolyte drink and transferring it to an insulated water bottle that would maintain a cold temperature of the drink. The best approach is to drink 250ml of fluids every 30mins and replenish fluids regularly. It is essential to slowly and continuously consume 150% of the fluid loss during competition within 120mins to improve the recovery process. Before exercising in the heat, it is important to drink 500-600ml of cold fluid an hour before the training or competition to improve the performance. Hyperhydration products are also often used before the exercise or competition as they increase body water content and storage by providing lots of sodium. This allows the body to enter competition or training with higher water content and this, in turn, increases the capacity of the body to absorb heat produced by working muscles that are then moved to the skin and removed as a sweat. This causes body core temperature to rise slower for the first hour of exercise. Pre-cooling by wearing ice vests, using fans, cold towels or baths, drinking frozen slushes also increases heat storage and allow athlete starts exercising with lower skin as well as body core temperatures giving them more time for efficient work before the temperature starts significantly rise.
For the subject in the present study, endurance training of 35min cycling at lactate threshold of 32-34ml/kg/min (corresponding to WR of 160W) three times per week with two interval sessions lasting 15min and two strength-training sessions would improve general cycling performance. In addition, AT was advised to the participant before she competed in Poland, in Autumn. The subject was advised to live in High Tatras (2200-2500m) and complete high-intensity training in Zakopane (750-1150m) for 4 weeks before the competition. The dietician advise was also given to the participant such as consuming extra minerals, fluids and sufficient amounts of CHO and fats. Moreover, the participant was advised to complete HA training before her event in Spain, in the summer. The subject has no access to heat chamber and no possibility to travel to Spain beforehand thus she was advised to complete 90min moderate-intensity cycling a day, with extra clothes on, in the hottest room in the house, for 14 consecutive days. She was also asked to have 30-40min hot water baths (40°C) straight after the cycling. This protocol also includes a gradual increase in WR each day (starting with 60W and finishing with 160W) and starts 3 weeks before the event to allow a week to easy any negative effects of the HA. The participant was also advised on proper hydration with electrolyte drinks and frozen slurries, wearing light and breathable clothing and any pre-cooling methods such as ice vest and cold towels or baths. Moreover, the participant was told to stop the HA training if she feels unwell to prevent any heat illness often starting with muscle cramps, heat exhaustion that can progress to heatstroke. Heat and altitude training both force athlete to workout in extreme and challenging conditions putting physiological stress on the body which, after some time, lead to physiological adaptations and performance improvements. However, HA is easier, more convenient and less expensive. It is important to avoid AT and HA together and plenty of time, preferable 21days, should be left between these two to allow body recovery. The competitions are few months apart thus both training methods were advised to the participant.
In the future, it would be beneficial to conduct invasive, direct lactate concentration testing by examination of blood samples at different points in the incremental exercise. This was proven to be the best method of determining blood LT (Bassett & Howley, 2000) and would give a better idea of the most accurate and reliable LT allowing to come up with the best training protocol. In addition, it would be beneficial to add some statistical analysis that would allow comparison of given results with other individuals. This would show variations between athletes.

Conclusion
In conclusion, measurement of VO2max is significant in exercise science as it is a determinant of the athlete’s fitness level, exercise capacity and the effectiveness of active training (Bassett & Howley 2000; Fletcher et al., 2001). Many studies have shown that well-trained athletes perform better compared to inexperienced or recreational athletes (Morgan & Craib, 1992). This suggests that exercise has a beneficial effect on people’s exercise capacity and significantly improve their VO2max, cardiovascular fitness and performance time. However, there are many interindividual variations in VO2max based on many factors such as cardiorespiratory system capability to provide O2 to the working muscles, muscles characteristics, maximal CO as well as running economy. Thus, it is necessary to determine VO2max for individual athletes to analyse the results and adapt their training programme accordingly. There are many VO2max limiting factors such as O2 carrying capacity, CO, pulmonary diffusion, blood flow, skeletal muscles’ characteristics. It is then necessary to take these factors into account when developing a training programme.
The findings from the present study show that VO2max can be predicted from the cycle ergometer exercise protocol with incremental intensity (Storer et al., 1990). It can be seen from the study that the maximum HR was reached (191bpm; Table 2) and the RER value (1.46; Figure 1) was within the norms for VO2max (1.15 or above). However, the VO2max was not fully achieved (37.21ml/kg/min; lower than participant’s absolute VO2max value of 41ml/kg/min) and only O2 uptake peak could be observed (Table 2 and 3) but due to the HR above the safe value, the experiment was terminated. However, the VO2 was not too far from the maximum value and other 2 criteria were met thus the experiment is classified as successful.
There are many ways of performance improvement. AT is still more often used way of improving the performance. However, HA is growing in popularity and may soon replace the AT. Both trainings improve performance by making biological adaptations in the body, such as improving cardiovascular system efficiency, metabolism, molecular responses, haemoglobin concentration, O2 carrying capacity, sweating rates, VO2max. However, HA, recurrent heat exposure of 90min per day for about 2 weeks sufficient for excessive sweating and body temperature rise, is more affordable and convenient.
Dig deeper into Maximizing Health Outcomes with our selection of articles.
REFERENCES
Armstrong, L.E., and Pandolf, K.B., 1988. Physical training, cardiorespiratory physical fitness and exercise-heat tolerance. In K.B. Pandolf, M.N. Sawka and R.R. Gonzalez (eds.) Human Performance Physiology and Environmental Medicine at Terrestrial Extremes. Benchmark Press, Indianapolis, IN, pp.199-226.
Astrand, I., 1960. Aerobic work capacity in men and women with special reference to age. Acta Physiologica, 49, pp.1-92.
Bang, O., 1936. The lactate content of the blood during and after muscular exercise in man. Skandinavisches Archiv Fur Physiologie, 74, pp.51-82.
Bassett, D. R. & Howley, E. T., 2000. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Medicine and Science in Sports and Exercise, 32, pp.70-84.
Bassett, D.R. & Howley, E.T., 1997. Maximal oxygen uptake: ''Classical'' versus ''contemporary'' viewpoints. Medicine and Science in Sports and Exercise, 29, pp.591-603.
Baumann, I., Bonov, P., Daniels, J., & Lange, G., 1994. NSA Round Table: high altitude training. New Studies in Athletics, 9(2), pp.23-35.
Beaver, W. L., Wasserman, K. & Whipp, B. J., 1986. A New Method for Detecting Anaerobic Threshold by Gas-Exchange. Journal of Applied Physiology, 60, pp.2020-2027.
Bishop, D., Jenkins, D. G., Mceniery, M. & Carey, M. F., 2000. Relationship between plasma lactate parameters and muscle characteristics in female cyclists. Medicine and Science in Sports and Exercise, 32, pp.1088-1093.
Bonetti, D.L., Hopkins, W.G., 2009. Sea-Level Exercise Performance Following Adaptation to Hypoxia. Sports Med, 39, pp.107–127.
Borg, G. A. V., 1982. Psychophysical Bases of Perceived Exertion. Medicine and Science in Sports and Exercise, 14, pp.377-381.
Branco, B. H., Massuça, L. M., Andreato, L. V., Marinho, B. F., Miarka, B., Monteiro, L., & Franchini, E., 2013. Association between the rating perceived exertion, heart rate and blood lactate in successive judo fights (randori). Asian journal of sports medicine, 4(2), p.125.
Carmichael Training Systems, nd. Beat the Heat Series: How to Prepare for Exercising in the Heat.
Available at:
Chapman, R.F., Stray-gundersen, J., & Levine, B.D., 1998. Individual variation in response to altitude training. Journal of applied physiology, 85(4), pp.1448-56 .
Chapman, R., Karlsen, T., Ge, R., Stray-Gundersen, J. and Levine, B., 2016. Living altitude influences endurance exercise performance change over time at altitude. Journal of Applied Physiology, 120(10), pp.1151-1158.
Day by Day coaching, 2015. How to cycle in extreme weather. Available at:
Dighe, R., 2017. 3 Ways to Heat Acclimatize When You Live in a Cold Climate. Available at:
Eichna, L.W., Park, C.E., Nelson, N., Horvath, S.M. and Palmes E.D., 1950. Thermal regulation during acclimatization in a hot, dry (desert type) environment. Am. J. Physiol, 163, pp.585-597.
Esfarjani, F. & Laursen, P. B., 2007. Manipulating high-intensity interval training: Effects on, the lactate threshold and 3000m running performance in moderately trained males. Journal of science and medicine in sport, 10(1), pp.27-35.
Fletcher, G., Balady, G., Amsterdam, E., Chaitman, B., Eckel, R., & Fleg, J. et al., 2001. Exercise Standards for Testing and Training. Circulation, 104(14), pp. 1694-1740.
Garvican-Lewis, L., Martin, D., McDonald, W. & Gore, C., 2010. Seasonal variation of haemoglobin mass in internationally competitive female road cyclists. European journal of applied physiology, 109, pp.221-31.
Gibbon, J., 2019. Beating the heat: How to ride in (and adjust to) hot conditions. Available at: < https://cyclingtips.com/2019/08/beating-the-heat-how-to-ride-in-and-adjust-to-hot-conditions /> [Accessed 11 April 2020].
Gonzalez, R.R. & Gagge, A.P., 1976. Warm discomfort and associated thermoregulatory changes during dry, and humid-heat acclimatization. Israeli J. Med. Sci, 12, pp.804-807.
Gore, C.J., Little, S.C., Hahn, A.G. et al., 1997. Reduced performance of male and female athletes at 580m altitude. European Journal of Applied Physiology, 75, pp.136–143.
Grant, S., Corbett, K., Amjad, A. M., Wilson, J. & Aitchison, T., 1995. A Comparison of Methods of Predicting Maximum Oxygen-Uptake. British Journal of Sports Medicine, 29, pp.147-152.
Hill, A. V., Long, C. N. H. & Lupton, H., 1924. Muscular exercise, lactic acid and the supply and utilisation of oxygen - Parts VII-VIII. Proceedings of the Royal Society of London Series B-Containing Papers of a Biological Character, 97, pp.155-176.
Karsten, B., Stevens, L., Colpus, M., Larumbe-Zabala, E., & Naclerio, F., 2016. The effects of sport-specific maximal strength and conditioning training on critical velocity, anaerobic running distance, and 5-km race performance. International journal of sports physiology and performance, 11(1), pp.80-85.
Kravitz, L. & Dalleck, L.C., 2002. Physiological factors limiting endurance exercise capacity: a thorough understanding of the components that limit performance in endurance exercise is crucial to designing effective programs for your clients. IDEA Health & Fitness Source, 20(4), p. 40.
Lorenzo S., Halliwill, J.R., Sawka, M.N. & Minson, C.T., 2010. Heat acclimation improves exercise performance. J. Appl. Physiol, 109, pp.1140-1147.
Mack, G.W. & Nadel, E.R., 1996. Body fluid balance during heat stress in humans. In: M.J. Fregly and C.M. Blatteis (eds.) Handbook of Physiology: Environmental Physiology, New York: Oxford University Press, Bethesda, MD: Am. Physiol. Soc., sect. 4, pp.187-214.
Mcardle, A. & Jackson, M.J., 2000. Exercise, oxidative stress and ageing. Journal of Anatomy, 197, pp.539-541.
Morgan, D. & Craib, M., 1992. Physiological aspects of running economy. Medicine & Science in Sports & Exercise, 24(4), pp.456-461.
Myers, J. & Ashley, E., 1997. Dangerous curves - A perspective on exercise, lactate, and the anaerobic threshold. Chest, 111, pp.787-795.
Nielsen, B., Hales, J.S.R., Strange, S., Christensen, N.J., Warberg, J. & Saltin, B., 1993. Human circulatory and thermoregulatory adaptations with heat acclimation and exercise in a hot, dry environment. J. Physiol. 460, pp.467-485.
Nieman, D., 2011. Heat acclimation improves exercise performance. Yearbook of Sports Medicine, 2011, pp.305-306.
Norm values for VO2max, 2019. Available at:
Nybo, L., Rasmussen, P. & Sawka, M.N., 2014. Performance in the heat-physiological factors of importance for hyperthermia-induced fatigue. Compr. Physiol, 4, pp.657-689.
Pandolf, K.B., 1998. Time course of heat acclimation and decay. Int. J. Sports Med. 19, pp.157-160.
Périard, J.D., Racinais, S. & Sawka, M.N., 2015. Adaptation and mechanisms of human heat acclimation. Scand. J. Med. Sci. Sports. 25, pp.20-38.
Poole, D. C., Wilkerson, D. P. & Jones, A. M., 2008. Validity of criteria for establishing maximal O-2 uptake during ramp exercise tests. European Journal of Applied Physiology, 102, pp.403-410.
Racinais S, Périard, J.D., Karlsen, A. & Nybo, L., 2015. Effect of heat and heat-acclimatization on cycling time-trial performance and pacing. Med. Sci. Sports Exerc. 47, pp.601-606.
Roberts, M., Wenger, C., Stolwijk, J., & Nadel, E., 1977. Skin blood flow and sweating changes following exercise training and heat acclimation. Journal of Applied Physiology, 43(1), pp.133-137.
Robertson, E.Y., Saunders, P.U., Pyne, D.B. et al., 2010. Reproducibility of performance changes to simulated live high/train low altitude. Medicine and Science in Sports and Exercise, 42(2), pp.394-401.
Sawka, M.N., Wenger, C.B. & Pandolf, K.B., 1996. Thermoregulatory responses to acute exercise-heat stress and heat acclimation. In: M.J. Fregly and C.M. Blatteis (eds) Handbook of Physiology, Section 4, Environmental Physiology. Oxford University Press, New York, Section 4, pp.157-185.
Sawka, M.N., Leon, L.R., Montain, S.J. & Sonna, L.A., 2011. Integrated physiological mechanisms of exercise performance, adaptation, and maladaptation to heat stress. Compr. Physiol, 1, pp.1883-1928.
Sawka, M.N., Périard, J.D., Racinais, S., 2016. Heat Acclimatization to Improve Athletic Performance in
Warm-Hot Environments. Available at:
Sawka, M.N., Cheuvront, S.N. & Kolka, M.A., 2003. Human adaptations to heat stress. In: H. Nose, G.W. Mack and K. Imaizumi (eds.) Exercise, Nutrition and Environmental Stress, Traverse City, MI: Cooper Publishing, 3, p.129-153
Schmidt, W., Heinicke, K., Rojas, J. et al., 2002. Blood volume and haemoglobin mass in endurance athletes from moderate altitude. Medicine and Science in Sports and Exercise, 34, pp.1934–1940.
Scoon, G.S., Hopkins, W.G., Mayhew, S. & Cotter J.D., 2007. Effect of post-exercise sauna bathing on the endurance performance of competitive male runners. J. Sci. Med. Sport, 10, pp.259-262.
Smyth, K., nd. Plan for The Heat. Available at:
Spurway, N. C., 1992. Aerobic Exercise, Anaerobic Exercise and The Lactate Threshold. British Medical Bulletin, 48, pp.569-591.
Storer, T., Davis, J., & Caiozzo, V., 1990. Accurate prediction of VO2max in cycle ergometry. Medicine & Science in Sports & Exercise, 22(5), pp.704-712.
Taylor, N.A., 2014. Human Heat Adaptation. Comprehensive Physiology, 4(1), pp.325-65.
Weller, A.S., Linnane, D.M., Jonkman, A.G. et al., 2007. Quantification of the decay and re-induction of heat acclimation in dry heat following 12 and 26 days without exposure to heat stress. Eur J Appl Physiol, 102, pp.57–66.
Weltman, A., 1995. The blood lactate response to exercise. Champaign, IL, Human Kinetics.
Wenger, H.A., Bell, G.J., 1986. The Interactions of Intensity, Frequency and Duration of Exercise Training in Altering Cardiorespiratory Fitness. Sports Medicine, 3, pp. 346–356.
Whipp, B. J., Davis, J. A., Torres, F. & Wasserman, K., 1981. A Test to Determine Parameters of Aerobic Function During Exercise. Journal of Applied Physiology, 50, pp.217-221.
Wilber, R.L., 2001. Current trends in altitude training. Sports Medicine, 31, pp.249–265.
Wilmore, J.H. & Costill, D.L., 2005. Physiology of Sport and Exercise. Harrogate: Human Kinetics.
Zurawlew, M.J., Walsh, N.P., Fortes, M.B. & Potter, C., 2016. Post‐exercise hot water immersion induces heat acclimation and improves endurance exercise performance in the heat. Scand J Med Sci Sports, 26, pp.745-754.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts