Texas BP Refinery Disaster
1. Introduction
In 2005, on 23rd March at the BP Refinery which was located at Texas city faced most worst blast in the industry of petroleum of the 21st Century. This is evident as nearly 15 people faced death and more than 180 individuals were severely injured as well as the company faced 1.5 billion monetary loss apart from their loss of reputation in the industry after the incident. The blast occurred after the hydrocarbon distillation process was initiated in the isomerised tower where the tower was over-filled leading to extensive formation of pressure which in turn led the relief valve get opened and sent combustible liquid splashes. This eventually led the explosive vapour cloud to get ignited from a nearby source of ignition (Saleh et al. 2014). On the day of the incident, the operators were seen to have initiated hydrocarbon fluid pumping to be to the splitting tower. The Tower in normal conditions is required to have 6 ½ feet fluid presence in the bottom with the two sensor installed for measuring the fluid height and another alarm being fitted for measuring the height above 10 feet. The completely mortalities were seen to have happened in the nearby trailers that were located near to the blowdown drum for delivering welfare facilities and meeting rooms for more than 1000 contractors who are seen to be working to maintain projects in the refinery apart from the management of employees at the place (Kalantarnia et al. 2010). I was appointed to examine the incidence for highlighting the timeline of critical events that contributed to the occurrence of the blast as well as discover the immediate reasons, modelling of the incidence on one of the causation model, mentioning duty of the leadership, culture, human factors, climate and ergonomics to prevent the accidents. In addition, I have to finally provide recommendations so that in future such incidences do not happen.

1.1 Scope and Approach
The aim in this report is to examine the explosion that occurred on the day of 23rd of March in the BP refinery in 2005 which is located in Texas. The examination of the operational documents and files were done and the recordings of the video for the day were checked. Moreover, interviews were conducted with the witnesses, operation contractors and individuals who were near the incidence. After the formation of the report with all evidence, it will be provided to the parties who are designated to keep the report.
2. Itinerary of Explosion and the events that led to the occurrence of the serious event
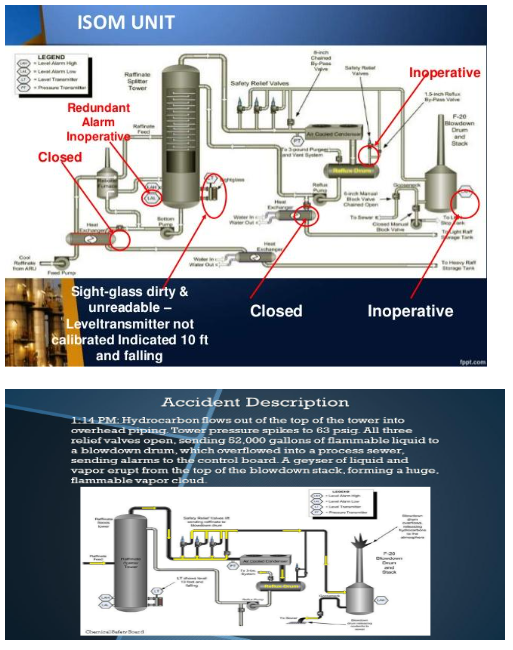
In 2005, on the day of 23rd March the explosion happened in certain part of the BP refinery that was concerning regarding raffinate spitter tower present in isomerzation unit (ISO) and blowdown system (Fig 1). A series of unfortunate events have resulted to the occurrence of this blast.
2.1 Key events initiated as follows
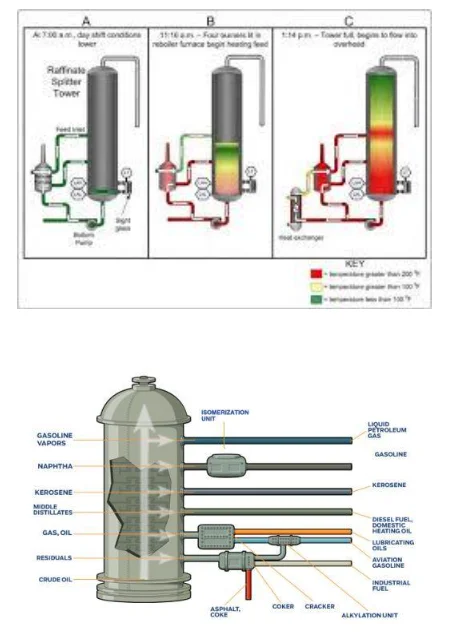
At 2.00 am on the mentioned date, normal and routinely operation has started where the workers produce hydrocarbons that are slightly imbustible in nature through the use of raffinate spitter tower (Fig 1). In the place, where the indicate is to pump 6.5 feet fluid at the lower part of the tower, a gauge is installed at the bottom region of the tower for measuring the amount of fluid present inside and later the data is sent to the control room. The gauge is developed in such a way so that it can be able to calculate maximum liquid of 10 feet in the tower but the operators cannot know if more than 10 feet of liquid is present in the tower or not by using this gauge. However, in this respect an alarm is fitted which indicates in the control room when the tower is filled over its specificity level as the alarm is triggered and buzz in the control room but there was an redundant alarm in addition which failed to work (Fig 4).
At 3.30 am, the filling of the liquid was stopped as the gauge level shows that 10 feet of the tower is filled with fluid from the bottom. However, the gauge was not seen to be showing the correct readings.
The main operator at 5:00 am updated the happening in the control room to the board operator and left his shift more that 1 hour before it ended.
A new board operator at 6:00 am arrived who was to initiate his straight shift for the 30th time and he go through the logbook in a brief manner. He found that there were no facts mentioned regarding the level of liquid to be present in the splitting tower.
The day shift supervisor arrived at 7:15 am and was late in his shift and mentioned her did not received any report or update related to the unit status.
At 9:50 am, the operators initiated the circulation of the fluid feet by forcing more fluid in the filled tower that is already full. The operator was unable to determine the fact as though more fluid was being poured there was no flow out as 10 minutes prior to the previous shit change the flow-out valves was closed.
At 10:00 am, the workers in the refinery ignited the burners for heating the liquid that is pumped in the tower. At this time, the staffs were not even aware that the tower is already 20 times excess filled than its usual capacity as the gauge being defective showed readings that the tower is filled below 10 feet and dropping.
By 11:00 am, the supervisor in the day shift has already left his charge due to a family emergency and in his absence no other experienced supervisor was present at the place which led the operation to be managed by inexperienced as well as unsupervised workers.
At 12:00 pm, the level of the liquid reached 98 feet high in the splitting tower however as a result of faulty gauge they showed 8feet high of the fluid that was dropping slowly.
At 12:40 pm, the alarm was triggered regarding high-pressure and the dual burner was switched-off for lowering the temperature of the fluid however valve which was controlling the pressure in the tower was not opened and the manual chain valve was opened by the worker for exhausting the gases to the blowdown drum which is to be then to the air.
At 1:00 pm, for reducing the pressure in the overfilled tower a valve ion the refinery was opened by the operators for sending fluid from tower base to tanks kept for storage purpose. However, the fluid being at high temperature when it was sent through the heat-exchanger, unfortunately it increased the temperature of the fluid more till 150 degrees.
At 1:05 pm, the pumped liquid in tower initiated boiling and expanding which caused the pressure and level of fluid to rise continuously.
At 1:10 pm, the fluid initiated to flow over to the piping present at the tower top and then was seen to build-up in the vertical piping that implemented extensive pressure on the three emergency relief vales present 150 feet lower.
At 1:14 pm, the liquid was flooding the blowdown drum after three emergency valves were already and then extended to the ISOM unit. This led the fluids flood the blowdrum in the process sewer and then the installed alarm did not go-off. The blowdown drum was entirely filled which resulted to flareup the fluids from the upper sacks to the bottom that generated a huge cloud of vapours which are flammable in nature.
At 1:20 pm, the ignition cloud of vapour produced contionous explosions which destroyed two trailers completely standing nearby killing 15 men and hurting more than 180 people with 150 chemical reservoirs destroyed (Fig 2 & 3). It is mentioned that the ignition sources came from a diesel pickup truck that has stopped at the place 25 minutes from the blowdown cylinder (csb.gov, 2007; propublica.org, 2010; Yang et al. 2016).
2.2 Root and Immediate causes
As per HSE 2014, root cause is referred to the initiating event or failing factor from which all other reason or failings are identified. However, the root causes are mainly the appearance of shortcoming of the management, planning and organisation whereas the immediate causes are representation of the noticeable reason regarding the occurrence of a serious incidence.
2.2.1 Root Causes
Lack of presence of programs for management of major risks and hazards
Extensively poor leadership and safety culture
Lack of adequate resources for avoiding negative incidences
Cutting of crucial budgets
Weak safety performance
Lack of proper reporting as well culture of learning such as mentioning band news to the authority for support and others
Investigation of incidents are not executed perfectly and no corrective actions were not taken
Absence of training programs to operate in the refinery
Low focus on personal safety and ignorance regarding safety process among workers
Absence of proper operational policies as well as procedures within the refinery plant
Improper and backdated designing of ISO unit
In the splitting tower, there was absence of automatic control for monitoring fluid level
Absence of proper supervision and direction by experienced supervisors
Absence of proper communication between employees during shift change
Absence of traffic policy for vehicles
Absence of effective management of site and trolley position and others (Samia et al. 2018; Scheberle, 2018; Shamim et al. 2018)
2.2.2 Immediate causes
Tired operations along with lack of tiredness remedy policies
Improperly designed control display and meters
Eroded level meters and gauges
Wrong operation
Poor and ineffective communications between the supervisors and operators during shift handover
Closed vent valve
High build up of pressure and overfilling of splitting tower
Non-operation of the emergency relief valves
Lack of experienced individuals during the failure of blowdown drum
Eruption of combustible liquid from the bottom
Diesel truck parked very near the place of the blowdown drum (Isimite and Rubini, 2016; Abílio Ramos et al. 2017; D'Andrea and Reddy, 2017; D’Andrea and Reddy, 2018)
3. Model of BP Texas Blast
The incident occurred in a complex way will be modelled with the help of a accident modelling tool named Reason Swiss Cheese Model (SCM) that is based on principles that accident occurs as a result of combination of various failures and factors (workplace, organisation and personal factors). Moreover, the model mentions different failure that is active and latent. The Active failure includes the unsafe practices that are able to be directly linked with the incident for instance the failure in operation at the plant. However, the latent failures inform the dormant failures that are present in the system for long time and contributes to cause the accident for example the failure of the equipments in the plant. In addition, for occurrence of adverse events the holes in the cheese slices are to be aligned while the barriers that are the defences of the organisation are hard and soft. The hard defences are the alarms and the soft defences are the training of employees, operation procedures and control of administration (Robinson, 2014; Elkind et al. 2011; Zio and Aven, 2013) The Fatal Accident Investigation Report 2005 informs that the incident may have been prevented or could have created slight impact but for 4 key reasons the disaster could not be avoided that includes unsuccessful initiation measures, loss of containment, improper application of skill and knowledge and improper management and control of trailers and work locations along with design of blowdown drum. In addition, the inlaid cultural factors such as poor working environment avoiding changing, lack of motivation and trust among employees, lack of power of employees and others. It was seen that safety was not a priority which is evident as the management at the place did not provide stress to reinforce proper safety measures, operations and practices. The lack of clear accountabilities to the staffs and improper communication along with high turnover of the upper management left the employees feel confused about their duties and role in the plant. The poor level of risk anticipation as a result of lower awareness and lack of familiarity with the process of safety and lastly the lack of early warnings as result of improper communication and training regarding management of correct standards of operation contributed to the accident. The management in BP were seen to avoid learning from past incidences. As per Kalantarnia et al. (2010), in past 10 years there are more that 6 near misses which include formation of cloud vapour due to spillage from same tower 2 times when they were shut down and 4 times other cases reported required intervention from the fire fighters. In addition, the management of BP has a poor confidence and safety regarding safety, intense and improper cutting of budgets, lack of presence of resources, management turnover, long working shifts, high management turnover that is 8 manager turnover from 2000 to 2005, lack of preventive measures at work and others (csb.gov, 2007). All the mentioned causes were seen to contribute in causing the explosion and will be presented in the Swiss Cheese Model below (Peek et al. 2009).


4. Theories of Culture, climate and leadership in the preventive accidents
In 2005, in BP the massive explosion took 15 lives and injury to 180 people and prior to this by the 32 years BP has experienced nearly 39 fatalities that when averaged shows 1 fatality per 16 months which is to be considered as one of the worst rate of accident in the US industry. In 2004, 3 of the fatalities that occurred have happened through 3 key accidents (Human factors, n.d.). The CSB (2007) informs that accidents have occurred as a result of organisational failure reasons that are rooted deep in the work culture, climate and safety management in the refinery. The poor management in the BP negatively influences the work culture for example the workers are encouraged to work in the plant by deviating from standard work procedures and use of faulty equipments along with improper inspection of alarms before executing work activities. This nature of work environment is shaped through improper motivation, bad expectation from the management and improper reward systems (Human factors, n.d). BP shows failure to develop a positive, open and trustworthy working environment with effective establishment of two-way communication between the management and workers all the time which results in cumulating of such accidents through the years (Peek et al. 2009).
4.1.1 Culture of Safety
The theory regarding safety culture that was developed in 1986 after the Chernobyl Disaster focuses on the human and organisational features which contributes to the operation of automated systems in unsafe way and defined as the role, norms, attitudes, beliefs and practices which work for reducing exposure of the employees to hazards at the workplace. It aims for development of norm in the staffs to become aware of risks and hazards at the workplace. Moreover, the safety culture informs and inspires safe behaviour by focussing on the attitudes and behaviour of the employees (HSE, 2008; Inkpen and Moffett, 2011; Coombs, 2013) (Fig 8).
4.1.2 Leadership of Safety
The safety leadership is referred as the communication between subordinates and leaders in which the leader uses their power to influence the subordinates for achieving safety goals of the organisation under individual and organisational elements (Peek et al. 2008).
4.1.3 Safety Climate
The safety climate mentions the attitude of the workers regarding safety in the organisation and it acts to indicate safety culture as accepted and understood by the employees. The psychological aspect of safety culture is mainly examined by questionnaires regarding safety climate that works to measure norms, attitudes, values and perception people regarding safety. However, in case of BP, it is found that they avoided addressing the above mentioned factors in serious manner with time that may have result them to build poor safety culture, reluctant safety leadership and poor climate of safety which contributed to increased number of accident, fatalities as well as misses. In order to reduce accidents in the BP, the management required to implement elements of positive safety leadership as well as effective two-way communication, learning among employees, discarding blaming culture, involvement as well as engagement of workers. The efficiently committed safety leadership is able to promote culture of safety by use of written and verbal communication. The verbal mode is to be used in establishing discussion within weekly meetings, training and organising safety tours whereas the written mode is to be used to provide safety information in the form of newsletter and declaration to the employees. Moreover, safety leadership can be able to influence risk perception of the employees by making them follow safety measures and complying with it as it would act as example for them to understand what the considerations to be made for managing safety. Thus, safety leadership while display a consistent behaviour and reaction for safety it is able to promote shared safety perception among the employees. The communication is required for all directions in the organisation from the management to the employees through the presence and implementation of clear safety policies, safety news, reporting of hazardous incidents and other negative issues that are to be seriously addressed while the horizontal communication is required to transferred safety information between departments, workers and employee groups (Rodríguez et al. 2011). The engagement and involvement of the workforce in proper training to increase their own safety, providing safety advice to employees by the specialist in managing safety, offer raise to the employees who show proper concern regarding safety at work act as significant point to avoid as well as control accidents and hazards at the workplace. The presence of culture of learning in the organisation to recognise, change and manage unsafe behaviour as well as conditions and inclusion of safety climate surveys to raise concerns regarding hazards are able to create an effective safety culture in the organisation. The organisation culture should not be a blame culture where the employees are held responsible for hazards but it is required to be just culture where the investigators has well understanding of the human errors happening in the organisation that are to be resolved to implement safety in the organisation. The investigator are required to know whom to assign the culpability and the way care as well as concern is to be showed to the employees for empowering them to freely report issues without having fear of getting blamed as unjustly treated (HSE, 2008).
In addition, the safe climate is been regarded as vital antecedent for safety performance in the work settings and it is regarded to have the ability of forecasting the safety behaviour and related outcomes at the workplace (Brizon and Wybo, 2009). As asserted by Saleh et al. (2014), it is found that the perceptions of the employees working in night shifts are lower regarding the perception between high-level and low-level safety climate. Thus, the employee to avoid injuries and accidents are to change their way of working when they perceive any nature of injury to be happening. In order to influence safe behaviour of the employees, presence of well committed safety supervisor and leadership is to be present at the workplace. They are also to be trained, provided simple job design, offered safety resources, learned to balance between productivity and safety at job and others (Robson, 2016).
5. Role of human factors, safe design and ergonomics in prevention of accident sin organisation
5.1 Human factors
The HSE (1999) refers that human factors are the organisational, environmental and job factors along with individual and human characteristics which is able to influence work behaviour in the way that it can influence the health and safety at work. The definition mainly contains three aspects that are individual, job and organisation that are to be collectively addressed and the way they are influencing behaviour of the people regarding safety and health. The job is required to be framed ergonomically where mental and physical capability of the employee is to be considered. In addition, the individual aspects which are attitude, personality and skills of the person that influences their behaviour are to be considered apart from culture in the organisation (Fig 6). Thus, human factors are the aspects that influence performance at the workplace (Zadakbar et al. 2015). Human factors are the multifaceted efforts which aim at collecting data regarding human abilities and their restrictions and application of the data for software, systems, procedure, staffing, training, personal management and facilities for obtaining a safe as well as effective human performance. In earlier time, human factors are implemented to obtain more profitability of better reliability, productivity, performance and safety (FSS, 2000). In the study of Wiegmann et al. (2007), it is informed that on the day of the accident the human factors that was responsible in creating the accident in BP is the working environment which accepted to work in unsafe culture. This is evident as over the 5 years out of 19 times it was seen that the tower was overfilled 15 times above the normal level. In addition, the procedures in work are changed improperly as the management at BP did not took into consideration change hazard analysis to manage the change as well as initiated to execute work operations without proper instructions. The lack of proper communication during shift change between supervisors to operators from day and night also contributed to the occurrence of the blast. The uncalibrated equipments and faulty instruments present on the tower that showed false levels and reading led the operators remain uninformed about the safety hazards. The improperly designed computer display failed to provide proper alarm for risks. Moreover, the lack of proper liquid balance display on the tower contributed to the accident.
The present of less experienced staffs at the control room to initiate the process contributed to the accident as the initiation of the process requires effective critical thinking as well as complex decision-making which was unable to be done by then present staffs. This lack of presence of experienced people is evident as only one experienced operator was controlling two units that mean huge workload on a single person as initiation and shut-down process requires to be managed by least two operators. The operators were also found to be fatigue due to long shifts for extends weeks making them unable to properly concentrate on maintaining proper safety during work. The poor training to the operators in the abnormal settings as well as lack of experience and qualifications, basic information delivery to execute work during on-job training and ineffective computer based training to the operators lead them to show weak performance in managing complex tasks resulting in the accident (CSB, 2007).
5.2 Ergonomics
Ergonomics is referred to ensure proper fit between equipments used and persons as physical and mental capabilities of the people different greatly (HSE, 1999). In addition, it includes the study to adjust the job to be done by the individual. Ergonomics is also concerned with designing of man-made machineries for leading the operators executes duties with fewer errors. For instance, at the workplace the displays are to be installed in such a way so that it can be used for easy scanning and proper choice of display type for facilitating dials and readings (Robson, 2016). In order to lower human errors as well as accidents, the organisations require lowering the stress regarding job among the employees at leads to increase errors. In addition, proper design and planning of plant and equipment is to be made and slips and lapses are to be reduced as well as proper supervision to experienced workers is to be offered to avoid accidents and safety issues at work (HSE, 1999).
6. Recommendations for preventing recurrence of events
The recommendations to be followed to avoid accidents and recurrence of hazards are as follows:
Developing a properly managed culture with effective and visible leadership
Offering a clarified system of chain of commands and accountability
Development of proper measurements for indicators regarding serious incidence
Arranging fatigue prevention programs
Offering ergonomically designed workplace and control rooms
Manage updated procedure of operation with continuous follow-up for start-up and shutdown process
Redesign of layout of the refinery for separating trailers and employees from hazardous process to safer places
Consideration of human factors for designing process or plant
Update of SDOM system
Compliance development with Process Safety requirement
Improving the alarm and sensor system (Wiegmann et al. 2007)

7. Conclusion
The above discussion informs that on 23rd March in 2005, explosion in the refinery of BP occurred that left 15 killed, 180 injured and led BP to loss 1.5 billion. A series of critical conditions led to the blast such as improper management, lack of safety procedures, use of faulty equipment and machineries, lack of safety leadership, improper budget cuts and others. The root causes include budget cuts, leadership and cultural hindrance in organisation, ineffective reporting of risks, lack of investigation of risks and others. The immediate causes include fatigue of the operators, faulty meters and gauges, operator errors and others. The root and immediate causes are identified by using Swiss Cheese Model. The human errors as well as ergonomics contributed to cause the blast at BP.



References
Abílio Ramos, M., Droguett, E.L., Mosleh, A., das Chagas Moura, M. and Ramos Martins, M., 2017. Revisiting past refinery accidents from a human reliability analysis perspective: The BP Texas City and the Chevron Richmond accidents. The Canadian Journal of Chemical Engineering, 95(12), pp.2293-2305.
Brizon, A. and Wybo, J.L., 2009. The life cycle of weak signals related to safety. International Journal of Emergency Management, 6(2), pp.117-135.
D’Andrea, M.A. and Reddy, G.K., 2018. Adverse health complaints of adults exposed to benzene after a flaring disaster at the BP Refinery Facility in Texas City, Texas. Disaster medicine and public health preparedness, 12(2), pp.232-240.
D'Andrea, M.A. and Reddy, G.K., 2017. Benzene exposure from the BP refinery flaring incident alters hematological and hepatic functions among smoking subjects. International journal of occupational medicine and environmental health, 30(6), pp.849-860.
Isimite, J. and Rubini, P., 2016. A dynamic HAZOP case study using the Texas City refinery explosion. Journal of loss prevention in the process industries, 40, pp.496-501.
Inkpen, A.C. and Moffett, M.H., 2011. The global oil & gas industry: management, strategy & finance. PennWell Books.
Kalantarnia, M., Khan, F. and Hawboldt, K., 2010. Modelling of BP Texas City refinery accident using dynamic risk assessment approach. Process Safety and Environmental Protection, 88(3), pp.191-199.
Peek, M.K., Cutchin, M.P., Freeman, D., Stowe, R.P. and Goodwin, J.S., 2009. Environmental hazards and stress: evidence from the Texas City Stress and Health Study. Journal of Epidemiology & Community Health, 63(10), pp.792-798.
Peek, M.K., Cutchin, M.P., Freeman, D.H., Perez, N.A. and Goodwin, J.S., 2008. Perceived health change in the aftermath of a petrochemical accident: an examination of pre-accident, within-accident, and post-accident variables. Journal of Epidemiology & Community Health, 62(2), pp.106-112.
Robinson, M.L., 2014. The tarnished BP brand: from Texas city to price fixing. In Marketing Big Oil: Brand Lessons from the World’s Largest Companies (pp. 64-70). Palgrave Macmillan, New York.
Rodríguez, J.M., Payne, S.C., Bergman, M.E. and Beus, J.M., 2011. The impact of the BP baker report. Journal of safety research, 42(3), pp.215-222.
Saleh, J.H., Haga, R.A., Favarò, F.M. and Bakolas, E., 2014. Texas City refinery accident: Case study in breakdown of defense-in-depth and violation of the safety–diagnosability principle in design. Engineering Failure Analysis, 36, pp.121-133.
Samia, C., Hamzi, R. and Chebila, M., 2018. Contribution of the lessons learned from oil refining accidents to the industrial risks assessment. Management of Environmental Quality: An International Journal, 29(4), pp.643-665.
Shamim, M.Y., Buang, A., Shariff, A.M. and Anjum, H., 2018. Implementation of Safety Performance Framework (SPF) In Process Industries to Avoid Disasters. International Journal of Automotive & Mechanical Engineering, 15(1).pp.90-99.
Wiegmann, D.A., von Thaden, T.L. and Gibbons, A.M., 2007. A review of safety culture theory and its potential application to traffic safety. Improving Traffic Safety Culture in the United States, 113.
Yang, H.N., Chen, J.H., Chiu, H.J., Kao, T.J., Tsai, H.Y. and Chen, J.R., 2016. Confined vapor explosion in Kaohsiung City–A detailed analysis of the tragedy in the harbor city. Journal of Loss Prevention in the Process Industries, 41, pp.107-120.
Zadakbar, O., Khan, F. and Imtiaz, S., 2015. Development of economic consequence methodology for process risk analysis. Risk Analysis, 35(4), pp.713-731.
Zio, E. and Aven, T., 2013. Industrial disasters: Extreme events, extremely rare. Some reflections on the treatment of uncertainties in the assessment of the associated risks. Process Safety and Environmental Protection, 91(1-2), pp.31-45.



What Makes Us Unique
- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts