Under-Five Mortality
Introduction
Under-five mortality has been defined by the World Health Organization as “the probability of a child born in a specific year or period dying before reaching the age of five, if subject to age-specific mortality rates of that period” (WHO, 2020a, p. 1). It is generally computed and reported as the number of children who die before their fifth year out of a thousand children born alive (Azuike et al., 2019; WHO, 2020a). The death of children before their fifth year is the foremost yardstick through which a country’s socioeconomic development and health system performance is rated (Nasejje et al., 2015; Gebretsadik and Gabreyohannes, 2016; Yaya et al., 2018a; Adewusi and Nwokocha, 2018). For those pursuing in-depth analysis on this topic, seeking healthcare dissertation help can provide valuable insights.
Compared to the situation about thirty years ago, global improvement has been made in terms of lessening the burden of under-five deaths (United Nations, 2015; Molyneux and Molyneux, 2016; WHO, 2018, UNICEF, 2019; WHO, 2020b). This is largely due to the increased attention given to this problem through the Millennium Development Goal (MDG) 4 (Bryce et al., 2013; United Nations, 2015; Yaya et al., 2018a; WHO, 2018). However, the current situation is still far from ideal. In 2017, more than 5 million under five deaths were recorded worldwide (Fikru et al., 2019). A similar figure was recorded in 2018 (UNICEF, 2019; WHO, 2020b).
Enormous differences have been reported in the occurrence of under-five deaths between developed countries and developing countries, with the latter bearing a disproportionate burden of this problem (Ayoade, 2018; Azuike et al., 2019; WHO, 2020b). Regional disparities have also been reported in the occurrence of these under-five deaths, with 76 compared to 9 children out of a thousand born alive at risk of dying before their fifth year of life in Africa and Europe respectively (WHO, 2020b). As a matter of fact, the Sub-Saharan African region alone accounted for about 50% of global under-five deaths in 2017 (Fikru et al., 2019) and 2018 (UNICEF, 2019), making it the world’s worst region in terms of under-five survival (Bitew and Nyarko, 2019; Andriano and Monden, 2019; Brault et al., 2020).
A vast majority of these Sub-Saharan African countries failed to achieve the under-five survival target set by MDG 4 (Nasejje et al., 2015; Brault et al., 2020). Nigeria is one of such countries with the rate of children dying before their fifth year of life still unacceptably high (Morakinyo and Fagbamigbe, 2017; Wegbom et al., 2019). World Bank Group (2019) reported that Nigeria had an under-five mortality rate of 120 deaths out of 1000 live births as at 2018. Consequently, Nigeria ranks among the ten countries with the highest rate of under-five deaths globally (Yaya et al., 2018b). However, the occurrence of these under-five deaths have been reported to be persistently unequal between regions and ethnic groups at country level (Adenini et al., 2015).

According to WHO (2019), a significant proportion of global deaths of children before their fifth year of life is due to largely avoidable causes such as pneumonia, malaria, and diarrhoea. Poor nutrition, overcrowding, inadequate breastfeeding, poor maternal healthcare access, poor vaccination uptake, poor water and food hygiene have been reported to be major risk factors for under-five mortality (WHO, 2019). According to Mosley and Chen’s (1984) framework, wider socioeconomic factors (individual-level, household-level, and community level) play a huge role in determining the direct medical causes of child mortality. These individual, household and community level socioeconomic factors include the mother’s education, household wealth and place of residence respectively (Mosley and Chen, 1984). Also, Mosley and Chen (1984) explained that a mother’s age determines child survival indirectly due to the effect it has on the reproductive health of the mother. Figure 1 below shows Mosley and Chen’s proximate determinants of child survival.

In most developing countries, young motherhood is highly associated with poverty and illiteracy and these act together to determine a child’s health (Finlay et al., 2011). Behavioural, cognitive and mental impairment is also reported to be more prevalent among children whose mothers are teenagers (Ayotunde et al., 2009). However, Ayotunde et al. (2009) found that while the likelihood of under-five mortality in Nigeria increased among mothers who are younger than 20 years, it also increased among mothers older than 35 years. Other Nigerian studies have reported conflicting results, with some reporting a lower likelihood of under-five mortality among younger mothers (Morakinyo and Fagbamigbe, 2017; Azuike et al., 2019), one reporting a reduced risk among mothers older than 25 years (Adekanmbi et al., 2015) and another reporting a reduced risk among mothers who are 35 and older (Wegbom et al., 2018).
A child’s survival chance has been said to be largely dependent on his/her mother’s education (Khurshid et al., 2019), based on the belief that more educated mothers are more likely to be better employed, earn more money, live in more healthy neighbourhoods and easily access quality healthcare for the child (Andriano and Monden, 2019). The higher likelihood of dying before the age of five for children of less educated mothers in Nigeria has been extensively reported (Adekanmbi et al., 2015; Ezeh et al., 2015; Morakinyo and Fagbamigbe, 2017; Koffi et al., 2017; Wegbom et al., 2018; Adewusi and Nwokocha, 2018; Ayinmoro et al., 2019; Azuike et al., 2019; Van Malderen et al., 2019). However, it has been argued that this relationship may not be as strong as the literature suggests and may be due to the effects of several confounders (Andriano and Monden, 2019). Hence, this epidemiological report aims to contribute to this body of knowledge by analysing secondary data obtained from the 2018 Demographic Health Survey (DHS) to find out if maternal education and age are risk factors for under-five mortality in Nigeria.
Methods
Data Source
Continue your journey with our comprehensive guide to Reliability Analysis and Professional Insights.
The secondary data used for this epidemiological report was obtained from the 2018 Demographic and Health Survey (DHS) program for Nigeria. The overarching aim of the Demographic and Health Survey program is to help international organizations and governments in planning and designing policies and programmes that will improve health outcomes through the collection and analysis of information about several health indicators and risk factors from large representative samples in many developing countries (Croft et al., 2018). The data was obtained after the submission of a short proposal indicating the aim of the report, the population to be studied and the variables to be measured.
Study Sample
A sample of 29,992 women who completed the DHS women’s questionnaire and indicated that they have had at least one child are included in this epidemiological report. All the women included are aged between 15 to 49 years. The DHS women’s questionnaire which was completed by the women will be submitted as an appendix along with this epidemiological report.
Variables
The independent variables for this epidemiological report are the highest educational level of the mother and the age of the mother. The mother’s highest educational level is divided into four categories which are, “no education”, “primary education”, “secondary education”, and “higher education”. The age of the mother is divided into three categories. The first category is between the ages of 15-27 labelled as “young aged”, The second category is between the ages of 28-37 labelled as “middle aged”, and the third category is between the ages of 38-49 labelled as “old aged”. The dependent variable in this epidemiological report is under-five mortality which is indicated by the loss (death) of a child before the age of five.
Statistical analysis
The data obtained was analysed using the Statistical Package for Social Sciences (SPSS) 26. Descriptive statistics were carried out to indicate the number (Frequency) and percentage of the respondents who lost a child before the age of five (shown in Table 1 below). A similar analysis was carried out to indicate the number (Frequency) and percentage of respondents by highest educational level (Shown in Table 2 below) and by age group (Shown in Table 3 below). Cross tabulation analysis was done to show the frequency of under-five mortality by highest educational level (Shown in Table 4 below) and age group (Shown in Table 5 below). Pearson’s Chi-square test was carried out to determine the significance of results.
Analysis was carried out to calculate the odds ratios for highest educational level and under-five mortality, using the fourth category “higher education” as the reference point or comparison (Shown in Table 6 below). Similar analysis was carried out to calculate the odds ratios for age group and under-five mortality, using the 15-27 age group as a reference point (Shown in Table 7 below). Lastly, logistic regression analysis was carried out to calculate the adjusted odds ratios for highest educational level and age group versus under-five mortality (Shown in Table 8 below). The results of the statistical analysis will be presented in the next section.
Results
Frequency and percentage of Under-five Mortality

Table 1 above presents the frequency and percentage of the respondents who lost a child before the age of five (Under-five mortality). Out of 29,992 respondents who reported ever having at least one child, 20,806 of them (69.4%) have never lost a child before the age of five while 9,186 of them (30.6%) have lost a child before the age of five.
Frequency and Percentage of respondents by Highest educational level
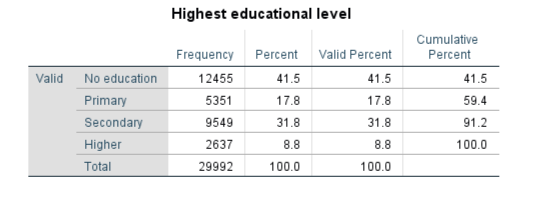
Table 2 above presents the frequency and percentage of respondents by highest educational level. Out of 29,992 respondents, 12,455 (41.5%) have no education, 5,351 (17.8%) have primary education, 9,549 (31.8%) have secondary education and 2,637 (8.8%) have higher education.
Frequency and percentage of respondents by age group

Table 3 above presents the frequency and percentage of respondents by age group. Out of 29,992 respondents, 9,554 (31.9%) are aged 15-27, 11,087 (37.0%) are aged 28-37 while 9,351 (31.2%) are aged 38-49 years.
Frequency of Under-five mortality by highest educational level

Table 4 above presents the frequency of under-five mortality by highest educational level. Out of 9,186 respondents who reported ever losing a child before the age of five, 5,347 (42.9%) have no education, 1,747 (32.6%) have primary education, 1,738 (18.2%) have secondary education while 354 (13.4%) have higher education.
Frequency of under-five mortality by age group

Table 5 above presents the frequency of under-five mortality by age group. Out of 9,186 respondents who reported ever losing a child before the age of five, 1,957 (20.5%) are between 15-27 years old, 3,522 (31.8%) are between 28-37 years old while 3,707 (39.6%) are between 38-49 years old.
Odds ratios for Highest educational level and Under-five Mortality

Table 6 above presents the odds ratios for highest educational level and under-five mortality. The likelihood of under-five mortality is highest for mothers with no education (Odds Ratio=4.85, 95% CI 4.31-5.46; p<0.001) compared to mothers with higher education. The likelihood of under-five mortality is higher for mothers with only primary education (Odds Ratio=3.13, 95% CI 2.76-3.54; p<0.001) compared to mothers with higher education. The likelihood of under-five mortality is high for mothers with only secondary education (Odds Ratio=1.43, 95% CI 1.27-1.62; p<0.001) compared to mothers with higher education.
Odds Ratios for Age group and Under-five Mortality

Table 7 above presents the odds ratios for age group and under-five mortality. The likelihood of under-five mortality is highest for mothers aged 38-49 years (Odds Ratio=2.55, 95% CI 2.39-2.72; p<0.001) compared to mothers aged 15-27 years. The likelihood of under-five mortality is higher for mothers aged 28-37 years (Odds Ratio=1.81, 95% CI 1.70-1.93; p<0.001) compared to mothers aged 15-27 years.
Adjusted Odds Ratios for Highest Educational level and Age group versus Under-five Mortality
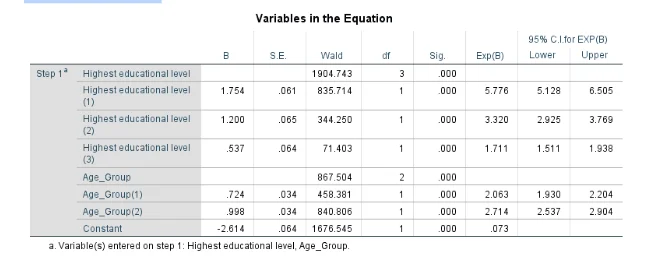
Table 8 above presents adjusted odds ratios for highest educational level and age group versus under-five mortality. After controlling for the effect of age, the likelihood of under-five mortality is still high for mothers with only secondary education (Odds Ratio=1.71, 95% CI 1.51-1.94; p<0.001), higher for mothers with only primary education (Odds Ratio=3.32, 95% CI 2.93-3.77; p<0.001), and highest for mothers with no education (Odds Ratio=5.78, 95% CI 5.13-6.51; p<0.001) compared to mothers with higher education. After controlling for the effect of highest educational level, the likelihood of under-five mortality is still higher for mothers aged 28-37 (Odd Ratio=2.06, 95% CI 1.93-2.20; p<0.001) and highest for mothers aged 38-49 (Odds Ratio=2.71, 95% CI 2.54-2.90) compared to mothers aged 15-27.
Discussion
Significance of Result
The results above show that maternal education and age are significant risk factors for under-five mortality in Nigeria. Children who are given birth to by mothers with no education have the highest likelihood of dying before their fifth birthday compared to children of mothers with higher education regardless of the mother’s age (Table 8). This agrees with the results of several studies (Adekanmbi et al., 2015; Ezeh et al., 2015; Morakinyo and Fagbamigbe, 2017; Koffi et al., 2017; Wegbom, Essi and Kiri, 2018; Adewusi and Nwokocha, 2018; Ayinmoro, Fayehun and Ogunsemoyin, 2019; Azuike et al., 2019; Van Malderen et al., 2019) which reported a similar relationship between maternal education and under-five mortality in Nigeria. Also, the results of this report show that children who are given birth to by older mothers (aged 38-49 years) have the highest likelihood of dying before their fifth birthday compared to children of young mothers (aged 15-27 years) in Nigeria regardless of the mother’s educational level (Table 8). This lends support to earlier findings by Morakinyo and Fagbamigbe (2017) and Azuike et al. (2019) who reported that the likelihood of under-five mortality is lower for children born to younger mothers. However, the results of this report may be confounded by other risk factors of under-five mortality such as household wealth and place of residence which were not included or measured in this epidemiological report.

Implications for Public Health
Nigeria was unable to meet the target of reducing under-five mortality set by Millennium Development Goal (MDG) 4 and major improvements are needed to achieve similar goals set by the Sustainable Development Goal (SDG) 3 (Durokifa and Abdul-Wasi, 2016). From the findings of this report, maternal education and age are significant risk factors for under-five mortality in Nigeria. Based on these findings, it is recommended that the efforts of government and third-sector bodies in reducing under-five mortality should include strategies aimed at supporting and improving the education of women. Furthermore, interventions aimed at improving the health of children should specially target older and uneducated mothers whose children are most likely to die before the age of five according to the findings of this report. Finally, more research should be carried out to ascertain the effects of other risk factors which were not studied in this report.
Strengths and Limitations of the Secondary Data
The Demographic and Health Survey (DHS) data collection process involves a rigorous calculation and sampling method to minimize sampling error and ensure that participants surveyed are representative of the larger population (Croft et al., 2018). Such rigorous sampling method is important in the reduction of selection bias (Coggon et al., 2003). Also, a major strength of the DHS data is that it is collected using standardized measuring instruments and methods along with the achievement of wide coverage and high response rates (Corsi et al., 2012). The use of standardized measuring instruments increases validity and reliability (Heale and Twycross, 2015). However, a major limitation of the DHS data is that most of the health indicators being measured are reported by the survey respondents themselves or by others on their behalf (Corsi et al., 2012). This makes such measurement prone to different types of self-reporting bias as some of the respondents may provide inaccurate answers to some of the questions being asked either intentionally or unintentionally (Althubaiti, 2016).
Conclusion
This epidemiological report has investigated the relationship between maternal education and age with under-five mortality in Nigeria by analysing secondary data obtained from the 2018 Demographic and Health Survey. Under-five mortality remains a significant public health problem in Nigeria. Maternal education and age have been widely reported as risk factors for under-five mortality in the literature. Similarly, this report found that maternal education and age are risk factors for under-five mortality in Nigeria, as children of uneducated mothers and older mothers had the highest likelihood of dying before the age of five. Hence, it is recommended that policies and strategies aimed at reducing under-five mortality in Nigeria should be designed in consideration of these risk factors.
REFERENCES
Coggon, D., Rose, G. A. and Barker, D. J. P. (2003) Epidemiology for the uninitiated. 5th Edition. London: BMJ Books.
Croft, T. N., Aileen, M. J. M., Courtney, K. A., et al., (2018) A Guide to DHS Statistics. Rockville: ICF.
Take a deeper dive into The Limitation of Summing Squared Loadings to Obtain Total Variance with our additional resources.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts