Research Methodology in Eating Disorder Studies
Introduction
Eating disorders have emerged as one of the leading health concerns among the youth that has diverse detrimental effects. Many studies have aimed to address this issue, various therapies have also been suggested as possible interventions for anorexia nervosa. Amongst them are the CBT-E and FBT. These studies have however failed to focus more on implementation of the therapy for adolescents aged 13-18 years. Besides, there lacks a better understanding of the problem and potential solutions. This makes the narrative critical. Thus, this study aims to answer the question: How effective is cognitive-behavioral therapy for adolescents suffering from eating disorders? To answer this research question, this dissertation undertakes review of literature to fill the gap that has been noted. The study begins with a background evaluation of the topic of examination followed by discussion of the research methodology, a brief presentation of the results, critical appraisal of the studies and final discussion of the findings and recommendations.
Chapter one
1.1 Define important concepts in the public health topic
Eating disorders usually affect how a person relates to food and their body image. Often the individuals spent most of their time preoccupied with thoughts of food and how it influences their body size, shape, and general image, (Walsh et al., 2020). They focus more on controlling their food intake rather than focusing on the benefit and health outcomes of eating. Anorexia nervosa is one of the food eating disorders characterized by weight loss, extreme dieting, starvation, or too much exercise. It primarily affects adolescent girls and young women with a disproportionately large ratio to the male of about 20:1, (Skowron et al., 2020).
1.2 Key international statistics
Statistical estimates show that at least 9% of the world’s population is affected by eating disorders accounting for about 70 people across the world living with this condition. Most of these are adolescents and young women with a median age of 18 years, (Santomauro et al., 2021). In Asia, Japan carries the highest prevalence with Singapore, South Korea, and Taiwan following suit. In Europe, Austria has the highest prevalence while almost 30 million people in America are said to live with the eating disorder. Women are more likely to develop the disorder than men, yet men are ones at a higher mortality rate mainly due to late diagnosis of the disorder. Moreover, the disorder is also more prevalent in older women with 13% of women above 50 years experiencing the eating disorder, (Nagata et al., 2018).
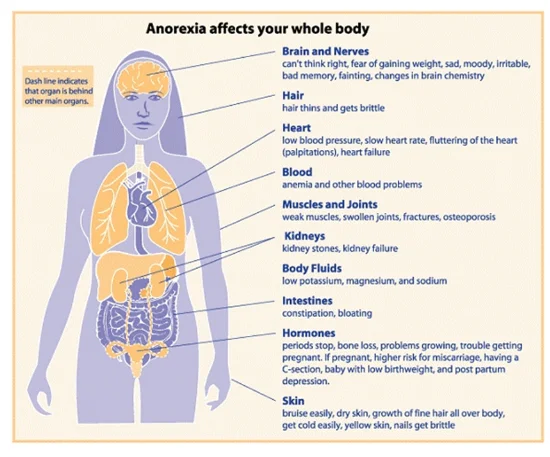
1.3 What are the health effects/impacts of the anorexia nervosa?
Continue your journey with our comprehensive guide to Depression and CBT.
The insufficient or even sometimes lack of adequate food intake leads to inadequate energy provision to the body of the patient. This in conjunction with the fact that the disorder is more common in adolescents whose organs are yet to be fully developed and that they have weight loss leads to a deterioration of not only the physical health of the patient but also the mental health. The disorder results in malnutrition that develops cause weight loss which if not checked leads to severe multi-organ failure. Furthermore, this is complicated by the fact that malnutrition leads to insufficiency of nutrient provision leading to endocrine dysfunction that will altogether ultimately lead to the death of the patient, (Walsh et al., 2020).
Dig deeper into Preventing NCDs in Adolescence with our selection of articles.
1.4 Key international policy/strategy
Various strategies can be adopted in the fight against eating disorders among the teenagers. Internationally, the scope for research strategies in the diversity and prevention of eating disorders has seen an enormous growth. The policy that has been suggested internationally involves a strategic plan that leverages the external environment for prevention as well as the full involvement of public health professionals that brings about a major choice of preventive stratagems and standpoints that are required in the curbing of the problem of anorexia nervosa. One of the policies is the National Eating Disorders Awareness Week that focuses on anorexia nervosa besides bettering the public understanding of factors that are related to the same. Another one is the Federal Response to Eliminate Eating Disorders Act that addresses the problem in a broad aspect. The act necessitates the director of the National Institute of Health to act regarding eating disorder research such as implementation of an approved budget on the research as well as the coordination and evaluation of NIH research activities and programs. They also target the expansion of NIH research on eating disorders and the establishment of a task force on anorexia nervosa and championing for the provision of centers for excellence for studies on anorexia nervosa (Pike et al., 2021).

1.5 Discuss and synthesise key risk factors and protective/preventive factors
Risk factors
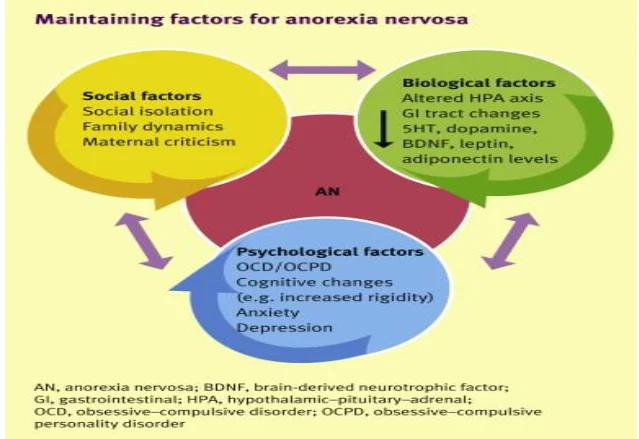
Risk factors too eating disorders can be categorised into genetic, psychological, and socio-cultural factors. Genetic factors are the susceptibility of an individual to inherit eating disorder from family lines (Pike et al., 2021). On the other hand, the psychological factors are inclusive of the behaviours and personality features that situate an individual at a higher risk of adopting disordered eating habits. The psychological factors are inclusive of stress, depression, and low self-esteem, avoidance of social interaction, trauma, and cynicism amongst other many factors (Pike et al., 2021). Socio-cultural factors are external or environmental activities that affect the perception of a person’s individual body (Figure 1). They also link to situations that are involving peers and friends. These factors are inclusive of peer pressure, bullying, societal pressure, and personal relationships (Pike et al., 2021).
1.6 Protective factors
These factors lower the possibility of an individual suffering from eating disorders. They have been grouped into individual, family, and socio-cultural protective factors. Individual factors include high self-esteem, positive body image, emotional well-being, school achievement, problem solving skills and emotional well-being (Pike et al., 2021). Family protective factors include originating from a family that emphasizes less on physical attractiveness and eating regular meals with the family. Socio-cultural protective factors entails coming from a less westernised culture that embraces distinct body shapes and sizes. Also, taking part in sport or any other area that does not focus much on physical attractiveness is a major socio-cultural protective factor (Pike et al., 2021).
1.7 Preventive Factors
Preventive measures are a form of primary prevention. One of the ways is creating awareness by educating the patients about nutrition. Another is health education and helping families communicate appropriately and guiding parents and guardians as well as children through the challenges of growth and individuation (Pike et al., 2021).
1.8 Perception of Target Population
Eating disorders are prevalent and life-threatening mental disorders. Research studies have indicated that people fail to seek treatment for the condition for fear of stigmatization. Besides, self-stigma has been identified as a factor that contributes to individuals avoiding treatment for anorexia nervosa. The public especially the adolescents have been reported to feel shameful when they realise they suffer from anorexia nervosa and other forms of eating disorders. Other has also reported with fear of change as a barrier to seeking treatment for the condition (Karas, 2014). Public opinion on eating disorders in the United Kingdom has noted various negative stereotypes that are related to anorexia nervosa. For instance, the public has termed anorexia nervosa patients as difficult to talk to, besides feeling different relative to other members of the public (Karas, 2014).
Looking for further insights on A Critical Analysis of a Prescribing Intervention? Click here.
1.9 Describe the key health promotion theories and relevant intervention method
As intervention method, Cognitive-based therapy is one of the psychotherapies currently being evaluated for use in the treatment of anorexia nervosa. It is, however, theoretically a relevant therapeutic modality for treating anorexia nervosa. It offers a long-term solution for the illness. Initially, the cause of anorexia nervosa was viewed to be unitary, however, current studies have shown that the disorder stems out of an array of etiological factors that are mostly different for each of the patients ("Cognitive behavioural therapy applied to anorexia nervosa and bulimia nervosa," 2018). As such other treatment modalities that view the etiological cause as being unitary fail to address why such modalities fail in different people. Cognitive-based therapy on the other hand, unlike the other modalities, views the disorder aetiology as multifocal and that treatment requires an understanding of the causal and maintaining variables that parallel its theoretical basis. Usually, the initiation of anorexia nervosa starts at the thought level and finally consumes a patient, and normally it is triggered by a certain past event thus the primary intervention should be to address the psychological issues of the disorder, ("Cognitive behavioural therapy applied to anorexia nervosa and bulimia nervosa," 2018). The health promotion theory emphasizes on assistance of people in attaining higher levels of wellbeing. Besides, it encourages health practitioners to offer positive resources that would be helpful to patients in achieving particular changes. They also help them in striving to control their own behaviour besides bettering their health and their environment. The health belief model is a theoretical model that guides health promotion as well as disease prevention programs. It thus not only explains but also predicts personalized changes in health behaviours. On the other hand, the cognitive model describes the influence of people’s thoughts and perceptions on their health through their feelings and behaviour’s (Pender, 2011).
1.10 Discuss the range of interventions
Psychological therapy
This is the most important intervention for treating eating disorders. Psychological therapy at the local level involves the patient visiting a psychologist or any mental health professional to help them in normalizing the eating patterns besides attaining a healthy weight. Also, therapists help anorexia nervosa patients to replace unhealthy habits for healthy ones as well as enabling them to learn ways of monitoring their eating as well as their moods (Reilly et al., 2017). There are three different kinds of therapies that can be applied for anorexia nervosa. The first is the cognitive behavioral therapy that involves a focus on the thoughts, behaviours, as well as the feelings that an individual have towards eating disorders. Cognitive behavioral therapy also assists the patient in recognizing and changing distorted thoughts that contribute to eating disorder symptoms. The other two types are the family-based therapy and the group cognitive behavioral therapy (Reilly et al., 2017).
Nutrition Education
Another promising intervention for anorexia nervosa is nutrition medication where registered dietitians alongside other professionals can take part in the treatment of eating disorder besides assisting the patient to develop a plan of attaining as well as maintaining healthy eating habits (Reilly et al., 2017). The various goals of this intervention are inclusive of working to attain a health weight, understanding the effect of nutrition on the body as well as being aware of how nutrition issues and physical problems are caused by eating disorders. Nutrition education also aims to establish regular eating patterns and correcting health issues which are caused by eating disorders such as anorexia nervosa (Reilly et al., 2017).
Medication for eating disorders
Medications can be used together with psychological therapy since they cannot treat eating disorders alone. The most common medications used are the antidepressants which are reduce the symptoms of depression or anxiety that are associated with eating disorders such as anorexia nervosa (Reilly et al., 2017). All these ranges are more effective when used together to treat eating disorders.
Chapter two
2.1 Literature Review Methodology
The study will adopt a secondary research approach. This would involve collecting data from published studies through systematic literature review. The research study will involve qualitative research design. The databases that will be used are inclusive of google scholars, PubMed, Medline, Medscape, Research gate, and Ebsco. Key words will be used to draw the relevant studies that will be reviewed. The key words to used include anorexia nervosa, eating disorders, cognitive behavioral therapy, teenagers, management, and effective. Boolean operators are used in combining the key words to limit the search. The research topic will also be used to source some studies. The studies will undergo an inclusion and exclusion criteria before they are used in the study. A critical appraisal tool will be used to critically appraise the studies for their quality and eligibility.
2.2 The importance and the definition of evidence-informed public health
Evidenced informed public health refers to the procedure whereby there is distillation and dissemination of the best available evidence from research as well as from practice and experience and making use of it in informing and improving public health policy and practice (Brownson et al., 2017) Thus, in my topic of study, evidence-informed public health would be essential in finding information from research and from practice where it would be shared and used in improving the health of adolescents suffering from anorexia nervosa.
2.3 PICO framework
This is a mnemonic that is applied in evidence-based practice in framing as well as answering a clinical and health related question. The following framework is used in this research study (Schardt et al., 2007). Summarised in appendix 1
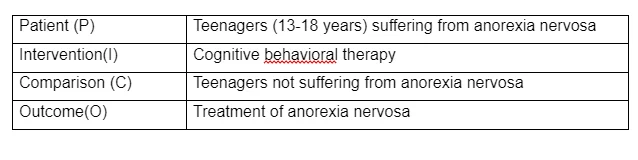
From the framework, the following key words were identified.
2.5 Inclusion and Exclusion Criteria
The studies that were included were those that evaluated cognitive behavioral therapy in teenagers, and they passed the following criteria:
Papers published in English and studies that reported human data Sample that met the for the definition of anorexia nervosa, as well as splurge-eating disorder and bulimia nervosa Studies with longitudinal design and original Experimental. Quasi-experimental, observational, controlled studies that discuss cognitive behavioral therapy in teenagers suffering from anorexia nervosa.
The criteria for exclusion were:
Non original and secondary reviews Cross-sectional studies
2.6 Literature review and Search Strategy
Literature review involves the summary, synthesis, and critique of literature that is found from literature search. The search for literature was not only designed but also undertaken. Databases were used and the PubMed database was first used since it has millions of references that are evidence-based and relevant to the topic of study. The database was screened in a systematic way using the MeSH terms that are listed; “anorexia nervosa (MeSH Terms) OR anorexia AND nervosa OR anorexia nervosa (All Areas) OR bulimia nervosa OR underweight (All Areas) OR not underweight nervosa (MeSH Terms) OR splurge-eating disorder (All Areas) (All Areas) OR splurge-eatings disorder nervosa (MeSH Terms) OR splurge eating disorders AND teenagers OR teenager OR teenage OR young population (All Areas) AND enhanced AND cognitive behavioral therapy nervosa (MeSH Terms) OR cognitive behavior therapy AND effects OR results” (All Areas) appendix4. Apart from the systematic screening, a manual free search was also undertaken in look for the terms that have been mentioned above as this helped in retrieving extra papers that were not identified through the initial search strategy that was used. Besides, the reference list of the sourced papers were assessed carefully in the quest to make sure that only the studies that were relevant to my study were identified. I did not consider the publication date as a criterion of excluding papers for the purposes of my literature review.
2.7 Refining and Narrowing of Literature Search
From a combined search of the databases, 110 research studies were identified. On reviewing the titles, 50 papers were removed as they were duplicates of each other. 32 papers were further removed as some were secondary reviews and others were cross-sectional studies. Of the 28 studies that remained, their references were examined, and 12 studies were removed as they were published more than ten years from the time of retrieval. 14 studies thus remained, and 8 more papers were removed since they did not meet the inclusion criteria completely. As a result, 6 research studies finally remained to be used in the review.
2.8 Data Collection and Data Items
I first undertook an independent assessment of the titles as well as the abstracts of the papers that I identified. This ensured the suitability of language as well as how relevant the papers were to my topic of examination. The papers that I identified in the study were then passed through an examination to ensure they were appropriate to be included in the study. Besides, their methodology was also assessed to ensure their appropriateness. The examination reviewed the authors, year that the papers were published, study design that the researchers adopted, sample size of the population that they examined, setting of the investigation, age, BMI of the participants, follow-up activities.
2.9 Critical Appraisal
Critical appraisal is the identification of possible threats to the validity of a research finding (s) from the literature besides offering consumers of research evidence for making informed decisions on the quality of the evidence from literature research. The critical appraisal is used to assess the quality of the studies for they to be used in the review. The UWL 9 question simple checklist has been used for critical appraisal of the research evidence. This tool ensures validity and reliability. Validity defines the integrity as well as the application of the undertaken methods as well as the precision such that the data are reflected by the data while reliability ensures consistency within the analytical procedures that have been used. it also ensures generalisability by ensuring that the findings can be generalized from the study sample to the general population. A summary table is included in the appendix 5.
2.10 Study Validity, Measurement reliability, and Generalisability
The study validity terms how well the results of this study represents true findings in similar individuals should the study be carried out outside the study (Leung, 2015). This is ensured alongside generalizability of the findings which refers to the measure of the usefulness of the results of the study in a larger group of people in similar situations. The results in this study are broadly applicable to diverse distinct kinds of individuals and situations thus it has a good generalizability (Leung, 2015). The reliability of the measurement in this study refers to how close the measurement procedures get to the actual quantity that the study aims to measure. This study has thus ensured that there is no measurement error. The critical appraisal has looked at the studies and has measured the validity of the measurement as well as its reliability, and generalizability of the research findings for each of the studies (Leung, 2015).
Definition and discussion of strengths and weaknesses of three main study designs
In article one, randomized controlled trial is used and it is better than the cohort study used in article to since it has a better generalizability of the study findings. Besides, if done correctly, randomized controlled trial is a better representation of the general population. Besides, the randomized controlled trial is an experimental approach for evaluating impact where the population that is undergoing an intervention is randomly chosen from an eligible population and there is also a control group that is equally chosen from the same population that is eligible. Its strength is that it minimizes biases and is comparative while it has weaknesses that concern logistics, statistics as well as its applicability. On the other hand, the cohort study used in article 2 and 3 involves research participants followed over a period of time and they share common features such as occupation of demographics. The strength is the longitudinal nature of data while the major weakness is that they are not good for rare disease unlike the condition under investigation.
Ethical considerations
These are a set of principles that guide the design as well as the practices of the research. The table below summarises the ethical issues of consideration in research studies.
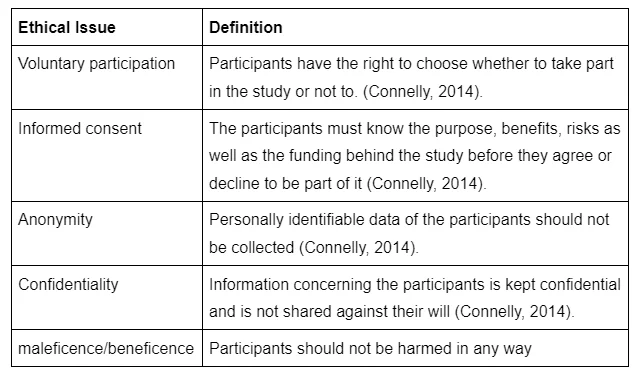
Ethics and ethical review matter when doing research for ensuring scientific integrity. Ensuring human rights is another important consideration besides ensuring human dignity and collaboration between science and the community at large. Thus, the research studies that would be reviewed must also have ethical approval as well as international good practice ethical principles. All the studies thus had ethical approval (Connelly, 2014). The studies have all discussed ethical approval as they had ethics review board. Participants’ ethics have been adhered to as ethical issues such as confidentiality and informed consent have been adhered to.
Chapter three
Critical Appraisal of Identified Studies
From the initial search, I was able to retrieve 20 papers. After exhaustive screening, seven papers were removed as they were inappropriate kind of papers. Four more papers were excluded as they only had adult patients and three more papers were removed using a generic form of CBT. After the final screening process, six papers were given consideration, as they were appropriate and suitable for the systematic review and narrative synthesis. Based on the NICE guideline, the selected studies ranged from good to bad in terms of their quality.
Article I
Clinical effectiveness of treatments for Anorexia Nervosa in adolescents: randomised controlled trial
Gowers et al., (2007) undertook a study to explore the effectiveness of anorexia nervosa in adolescents. The researchers conducted a randomized controlled trial that aimed to draw a comparison of the clinical effectiveness of in-patient against specialist out-patient as well as the treatment in the community On the other hand, there were no exclusions that were made based on clinical severity. The recruitment approach involved identification of patients that had possibilities of suffering from anorexia nervosa. The young participants were then interviewed, and diagnosis was confirmed before an informed consent of participation in the trial was conducted. One of the treatments that was provided was inclusive of an in-patient psychiatric treatment which was offered to generic children and adolescent psychiatric in-patient units. Also, this involved the usage of a multidisciplinary psychiatric approach that aimed to normalize eating. There was an anticipated weight increase of 0.8kg to 1kg on a weekly basis. Apart from that treatment, there was also a specialized out-patient treatment program that consisted of two services. Another treatment that was provided by the researchers was general community CAMHS that was not manualized and involved 35 services. Measures that the researchers undertook included interviewer-based measures, participant’s ratings, amongst other ratings. The results from the study indicated an increased weight of the participants and reduction in the pathology of anorexia nervosa. This was thus an indication of the effectiveness of cognitive behavioral therapy in the treatment of anorexia nervosa (Gowers et al., 2007). Gowers, S., Clark, A., Roberts, C., Griffiths, A., Edwards, V., Bryan, C., Smethurst, N., Byford, S. and Barrett, B. (2007) Clinical effectiveness of treatments for anorexia nervosa in adolescents. British Journal of Psychiatry, 191(5), pp.427-435.
Article II
Enhanced cognitive behavioral therapy for adolescents with anorexia nervosa: Outcomes and predictors of change in a real-world setting
In 2019, Dalle Grave et al. undertook a different study and they aimed to know the results as well as the predictors of change in a group of teenagers with anorexia nervosa that were treated through an outpatient cognitive behavioral therapy in a hospital setting. The researchers made an assessment of 99 patients for their eligibility. From the assessment, 49 patients were enrolled for the study. This means that 50 patients were excluded from the study. Of the 50, 30 failed to meet the inclusion criteria while 18 of them met the exclusion criteria. Two of the 50 refused to take part in the study. The teenagers who were selected had a mean age if 15.5 years while their mean BMI-for-age percentile was 5.67 at the beginning of the treatment. They had suffered from the condition for a mean period of 0.95 years. The full sessions constituted of 40 sessions of cognitive behavioral therapy and 35 patients completed the sessions. Of the 35 patients, 29 of them took part in follow up activities that were conducted thereafter after 20 weeks. The results from the study indicated that there was a substantial increase in the BMI-for-age percentile as the treatment progressed. However, during the follow-up activities, a significant deceleration was noted. Over the treatment, there was also a reduction in eating disorder as well as the general psychopathology and, clinical impairment of the patients that took part in the study. The parameters continued to improve as time progressed up to the follow up that took place in the 20th week. After the program, 22 of the participants that took part in the treatment program had a BMI-for-age percentile that corresponded to that of an adult that was more than 18.5kg/m2. The results by the researchers were attained in 48.3% of the 29 participants that took part in the follow-up for 20 weeks (Dalle Grave, Sartirana and Calugi, 2019). Dalle Grave, R., Sartirana, M. and Calugi, S. (2019) Enhanced cognitive behavioral therapy for adolescents with anorexia nervosa: Outcomes and predictors of change in a real‐world setting. International Journal of Eating Disorders, 52(9), pp.1042-1046.
Article III
Optimising treatment outcomes in adolescents with eating disorders: The potential role of cognitive behavioral therapy
In the same year, Craig et al. wrote a title that explored the optimization of treatment outcomes in adolescents suffering from anorexia nervosa and the role that cognitive behavioral therapy in addressing eating disorders. The researchers noted that family-based treatment is the most commonly used psychological therapy in the treatment of anorexia nervosa among the adolescents. However, they also took note of the fact that FBT id universally ineffective and unsuitable. The study made a consideration of the effectiveness that cognitive behavioral therapy has in anorexia nervosa in adolescents in cases that FBT was not as effective as desired. The study involved a transdiagnostic case series that involved 54 adolescents whereby 52% of them were suffering from anorexia nervosa while 31% were suffering from atypical anorexia nervosa. The participants underwent CBT-ED after being treated with FBT and after FBT was inappropriately judged. The authors also used pre-post outcomes assessment through standardized measures of eating attitudes as well as clinical impairment and measurements of weight changed were taken. From the study, the researchers noted that the patients who took part in the study showed a positive result in all the measures that were taken. Besides effect, sizes were also noted to range from moderate to large. The outcomes had no link to duration as well as the severity of eating disorders of the patients (Craig, Waine, Wilson and Waller, 2019). Craig, M., Waine, J., Wilson, S. and Waller, G. (2019) Optimizing treatment outcomes in adolescents with eating disorders: The potential role of cognitive behavioral therapy. International Journal of Eating Disorders, 52(5), pp.538-542.
Article IV
Inpatient Cognitive Behaviour Therapy for Adolescents with Anorexia Nervosa: Immediate and Longer-Term Effects
Dale Grave et al. undertook a study in 2014 that examined the effectiveness of inpatient CBT-E in a sample of adolescents that had been diagnosed with eating disorders. This assessment was undertaken at the end of the treatment at time intervals of 6 months and after a year that comprised of follow up activities. The researchers found 32 patients that were eligible to take part in the evaluation. Of the 32, only 27 of them agreed to be part of the research study. The 27 participants competed the treatment program while 22 and 23 of them respectively took part in the follow-up activities that were undertaken after 6 months and 12 months of treatment. Intention-to-eat analysis was also carried out by the researchers and a surge in the BMI of the participants was reported in BMI percentile from the initial baseline to the when the treatment was completed. The BMI percentile was reported to have been27.3 and 29.9 after 6 months and 12 months respectively. Besides, the researchers carried out a completer analysis that indicated similar results. Particularly, a BMI percentile from the completer analysis was noted to be 35.5 when the treatment ended and 25.4 and 29.5 at 6 months and 12 months after treatment respectively. Among the completers that were evaluated, a good number of them attained a BMI percentile that aligned to a BM I of more than 18.5 when the treatment was complete. On the other hand, 82.6% of the completers had a BMI percentile that was corresponding to more than 18.5 at the time when a follow-up activity was being carried out in the twelfth month after treatment was completed. Also, the pathophysiology of anorexia nervosa saw a significant decrease with a remarkable percentage of 38.5, 59.1, and 60.9 at the end of treatment, after 6 months follow-up and 12 months follow-up activities respectively. The results from this study also indicated the effectiveness of cognitive behavioral therapy in the treatment of anorexia nervosa among adolescents (Dalle Grave et al., 2014). Dalle Grave, R., Calugi, S., El Ghoch, M., Conti, M. and Fairburn, C. (2014) Inpatient Cognitive Behavior Therapy for Adolescents with Anorexia Nervosa: Immediate and Longer-Term Effects. Frontiers in Psychiatry, 5(14), pp.1-7.
Article V
Enhanced cognitive behaviour therapy for adolescents with anorexia nervosa: An alternative to family therapy?
In 2013, a study was undertaken by Dalle Grave et al that explored the effectiveness of outpatient CBT-E in combating anorexia nervosa among the teenagers. The study involved a cohort of 49 adolescent patients that were diagnosed with anorexia nervosa and were referred tan clinic that assists patients with eating disorders. Of the patients that took part in the study, only three of them that was a 6.1% representation refused taking part in the cognitive behavioral therapy. Of the 46 participants that agreed to be part of the study, 29 of them went through with it and completed the study. Also, they all took part in the follow-up activities that were conducted 60 weeks from the time the therapy ended. During this study, the researchers also carried an intention-to-eat analysis that indicated a significant increase in BMI-for-age percentile that surged from the preliminary 2.86 at the start of the treatment to 19.8 when the treatment came to an end. At the end of the follow-up activity after 60 weeks, the BMI had risen to a remarkable 23.6. Besides, a good number of the patients that took part in the study recorded a substantial increase in their weights. For instance, they achieved 95% of their expected weight. The psychopathology of anorexia nervosa also decreased from 2.79 to 1.50 at the beginning and end of the therapy program respectively. It was 1.51 at the end of the follow up activity. More than 70% of the participants attained a universal EDE-Q of more than 1SD that was noted to be more than the mean of the community when the treatment ended as well as at the end of the follow-up activity after 60 weeks. Also, the psychiatric features that were initially noted in the patients also saw a decline from the time when the treatment to the time when it came to an end and the end of the follow-up activities (Dalle Grave, Calugi, Doll and Fairburn, 2013). Dalle Grave, R., Calugi, S., Doll, H. and Fairburn, C. (2013) Enhanced cognitive behaviour therapy for adolescents with anorexia nervosa: An alternative to family therapy? Behaviour Research and Therapy, 51(1), pp. R9-R12.
Article VI
Three Psychotherapies for Anorexia Nervosa: A Randomized, Controlled Trial
The last study that I found was an article by Virginia et al. and the study was carried out in 2005 to examine the three psychotherapies for anorexia nervosa through a randomized and controlled trial. The methodology was used in examination of the efficacy of treatments for anorexia nervosa. The treatments involved cognitive behavioral therapy as well as interpersonal psychotherapy and they were been assessed whether they were effective in a related disorder and bulimia nervosa. The study involved 56 women that were suffering from anorexia nervosa. Their conditions were diagnosed via not only strict but also lenient weight criteria that were assigned to three treatments in a random manner. Two of the treatments included specialized psychotherapies while the other treatment was a control treatment that involved a combination of clinical management as well as supportive psychotherapy. From the research study, substantial differences were noted between the therapies that the participants were subjected to. Nonspecific supportive clinical management was more significant relative to interpersonal psychotherapy. Also, the researchers noted that cognitive behavioral therapy was in between the other therapies in terms of effectiveness. The results of the study supported the effectiveness of CBT-E in anorexia nervosa (McIntosh et al., 2005). McIntosh, V., Jordan, J., Carter, F., Luty, S., McKenzie, J., Bulik, C., Frampton, C. and Joyce, P., (2005). Three Psychotherapies for Anorexia Nervosa: A Randomized, Controlled Trial. American Journal of Psychiatry, 162(4), pp.741-747.
Chapter four
Expand the details of the interventions used in each of the articles
Article 1
In the first study, the interventions that the researchers considered for the study sample included an in-patient psychiatric treatment which was offered to generic children and adolescent psychiatric in-patient units. Also, this involved the usage of a multidisciplinary psychiatric approach that aimed to normalize eating. There was an expected weight increase of 0.8kg to 1kg on a weekly basis. Apart from that treatment, there was also a specialized out-patient treatment program that consisted of two services. Another treatment that was provided by the researchers was general community CAMHS that was not manualized and involved 35 services. Measures that the researchers undertook included interviewer-based measures, participant’s ratings, amongst other ratings (Growers et al., 2007).
Article 2
In the second article, the specific interventions involved an outpatient cognitive behavioral therapy within a hospital setting. There was a substantial increase in the BMI-for-age percentile as the treatment progressed (Dalle Grave et al., 2019).
Article 3
The third article also involved both family-based treatment and enhanced cognitive behavioral therapy. There was a positive result in the measures such as BMI that were undertaken. . The participants underwent CBT-ED after being treated with FBT and after FBT was inappropriately judged. The authors also used pre-post outcomes assessment through standardized measures of eating attitudes as well as clinical impairment and measurements of weight changed were taken. From the study, the researchers noted that the patients who took part in the study showed a positive result in all the measures that were taken. Besides effect, sizes were also noted to range from moderate to large (Craig et al., 2019).
Article 4
In the fourth study, an inpatient behavioral therapy intervention was used. Intention-to-eat analysis was also carried out by the researchers and a surge in the BMI of the participants was reported in BMI percentile from the initial baseline to the when the treatment was completed (Dalle Grave et al., 2014).
Article 5
The researchers used enhanced cognitive behavioral therapy. The researchers also carried an intention-to-eat analysis that indicated a significant increase in BMI-for-age percentile that surged from the preliminary 2.86 at the start of the treatment to 19.8 when the treatment came to an end. The BMI had risen to a remarkable 23.6. Besides, a good number of the patients that took part in the study recorded a substantial increase in their weights (Dalle Grave et al., 2014)
Article 6
The sixth article involved three psychotherapies that included cognitive behavioral therapy, family-based therapy as well as interpersonal behavioral therapy. All the six articles noted that enhanced cognitive behavioral therapy is the most effective for anorexia nervosa treatment. Two of the treatments included specialized psychotherapies while the other treatment was a control treatment that involved a combination of clinical management as well as supportive psychotherapy. From the research study, substantial differences were noted between the therapies that the participants were subjected to. Nonspecific supportive clinical management was more significant relative to interpersonal psychotherapy (McIntosh et al., 2006)

Discussion
Article 1
CBT-E is adequately effective for adolescents relative to adults that suffer from eating disorder. One of the studies that were reviewed compared the effectiveness of CBT-E in adolescents and adults and reported that there was a significantly higher percentage of teenagers that attained normal weight when they were compared to the adults at the end of the treatment as the percentages were 65.3% and 36.5% respectively. Besides, the researchers noted that adolescents needed shorter mean time to attain normal weight relative to the adults that were suffering from anorexia nervosa. CBT-E has also been noted to be specifically effective when applied for adolescents suffering from eating disorders in an inpatient setting and was also used in treatment of patients that were severe and medically unstable.
Article 2
In the group of patients that were severely ill, 80% of them attained a normal weight while approximately 50% saw the remission of anorexia nervosa to completion one year after the end of the treatment (Calugi et al., 2015). The adults as well as the adolescents that were treated with inpatient CBT-E had similar outcomes at the beginning as well as at the end of the treatment. This was not the case for the adults and adolescents that were treated with outpatient CBT-E (Dalle Grave et al., 2020).
Article 3
The findings from the studies that are systematically reviewed are in support of the idea that CBT-E is effective in the treatment of anorexia nervosa among adolescents. Two clinical studies that have been explored assessed the effectiveness of outpatient CBT-E for adolescents with eating disorders and reported that the treatment of anorexia nervosa through the cognitive behavior therapy. Besides, they noted that the treatment is well accepted and in most of the research studies, at least 66.7% of the sample size accepted to take part in the trials. Besides, it was linked to substantial surge in the BMI-for-age percentile as well as enormous improvements in the pathophysiology of eating disorders alongside the general pathophysiology scores. The improvements were subsequently maintained during the follow-up activities that were carried out at either the 20th or the 60th week or both in some of the research studies that have been reviewed for this systematic review. Notably, from the individuals who completed the trials and the follow-up activities thereafter, 50% equally attained complete remission from eating disorders.
Article 4
For the not-underweight adolescents, the data for the effectiveness of CBT-E for the outpatient was limited. One study by Dalle Grave et al. (2014) did an assessment of the effectiveness for outpatient CBT-E in adolescent patients that were suffering from bulimia nervosa as well as in those that were suffering from binge-eating disorder or any other eating disorder. The findings by the researchers from the study showed that three-quarters of the participants saw the treatment to completion. Besides, more than half of the participants that were suffering from binge-eating disorder stopped such behaviors when the treatment came to completion (Dalle Grave et al., 2015). Of those that completed the treatment, 80% of them reported with reduced residual eating-disorder psychopathology when the treatment came to completion.
Article 5
All the three studies by Dallle Grave et al. that have been reviewed in the research study assessed the effectiveness of inpatient CBT-E and noted that the treatment was well accepted besides being completed by 90% of the patients. Just like the outpatients that used the therapy, the inpatients also had a substantially heightened BMI-for-age percentile besides having an increased improvement in general pathophysiology scores as well as the eating disorder pathophysiology (Dalle Grave et al., 2019; Dalle Grave et al., 2020; Dalle Grave et al., 2014). These were similarly maintained during the follow up activities after 20 weeks and after 60 weeks.
Article 6
One of the studies that have been reviewed made a comparison of CBT-E with a different form of treatment for adolescents with eating disorders. The study was undertaken by McIntosh et al. in 2006 and involved a non-randomized trial that made a comparison of ten relative effectiveness of CBT-E and FBT in adolescents that were categorized into treatment groups based on the preference and further divided into lower weight group and higher weight group. From the study, the researchers noted that FBT was relatively more effective compared to CBT-E as much as weight gain was concerned from the beginning to the end of the treatment. There was however no significant difference between the two forms of treatment at the 6th month and the 12th month of follow-up activities. All the studies that have been reviewed are in support of the effectiveness of CBT-E for adolescents suffering from eating disorders. The therapy has been noted to be well accepted by the patients as well as their parents. It should thus be considered in the management of anorexia nervosa across the world (Calugi et al., 2015). It can be recommended that further research be undertaken on the issue to better understand how other therapies are helpful min treating anorexia nervosa. Also, it is recommended that future research be focused on other therapies as well as other types of eating disorders.
Conclusion
Anorexia Nervosa has a negative impact on the physical as well as the psychosocial health of adolescents suffering from the disease as well as their families. Such disorders have been linked with other mental conditions such as suicidality and role impairment. This literature review has assessed the effectiveness of cognitive behavioral therapy among adolescents with eating disorders. The study adopted a secondary research approach. Data has thus been collected from published studies through systematic literature review. The study has noted that CBT-E is more effective for treating eating disorders in adolescents relative to FBT. It is well accepted by both patients and their parents. Improvements are noted after six months and twelve months follow-up activities.
References
- Brownson, R. C., Baker, E. A., Deshpande, A. D., & Gillespie, K. N. (2017). Evidence-based public health. Oxford university press.
- Connelly, L. M. (2014). Ethical considerations in research studies. Medsurg Nursing, 23(1), 54-56.
- Craig, M., Waine, J., Wilson, S. and Waller, G., (2019). Optimizing treatment outcomes in adolescents with eating disorders: The potential role of cognitive behavioral therapy. International Journal of Eating Disorders, 52(5), pp.538-542.
- Dalle Grave, R., Calugi, S., Doll, H. and Fairburn, C., (2013). Enhanced cognitive behaviour therapy for adolescents with anorexia nervosa: An alternative to family therapy? Behaviour Research and Therapy, 51(1), pp. R9-R12.
- Dalle Grave, R., Calugi, S., El Ghoch, M., Conti, M. and Fairburn, C., (2014). Inpatient Cognitive Behavior Therapy for Adolescents with Anorexia Nervosa: Immediate and Longer-Term Effects. Frontiers in Psychiatry, 5(14), pp1-7.
- Dalle Grave, R., Sartirana, M. and Calugi, S. (2019) Enhanced cognitive behavioral therapy for adolescents with anorexia nervosa: Outcomes and predictors of change in a real‐world setting. International Journal of Eating Disorders, 52(9), pp.1042-1046.
- Gumz, A., Weigel, A., Wegscheider, K., Romer, G., & Löwe, B. (2018). The psychenet public health intervention for anorexia nervosa: a pre–post-evaluation study in a female patient sample. Primary health care research & development, 19(1), 42-52.
- Karas, K. (2014). Public perceptions of anorexia nervosa (Doctoral dissertation, The University of Wisconsin-Milwaukee).
- Leung, L. (2015). Validity, reliability, and generalizability in qualitative research. Journal of family medicine and primary care, 4(3), 324.
- McIntosh, V., Jordan, J., Carter, F., Luty, S., McKenzie, J., Bulik, C., Frampton, C. and Joyce, P., (2005). Three Psychotherapies for Anorexia Nervosa: A Randomized, Controlled Trial. American Journal of Psychiatry, 162(4), pp.741-747.
- Reilly, E. E., Anderson, L. M., Gorrell, S., Schaumberg, K., & Anderson, D. A. (2017). Expanding exposure‐based interventions for eating disorders. International Journal of Eating Disorders, 50(10), 1137-1141.
- Schardt, C., Adams, M. B., Owens, T., Keitz, S., & Fontelo, P. (2007). Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC medical informatics and decision making, 7(1), 1-6.
- Pike, K. M., So, M., Hilbert, A., Maekawa, H., Shimanouchi, T., Wilfley, D., ... & Weissman, R. S. (2021). Risk factors for anorexia nervosa and bulimia nervosa in Japan and compared to a US sample. International Journal of Eating Disorders, 54(2), 155-167.
- Woerwag-Mehta, S. and Treasure, J. (2008) Causes of anorexia nervosa. Psychiatry, 7(4), pp. 147-151. doi:10.1016/j.mppsy.2008.02.010



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts