Why Sickle Cell Must Be a Global Health Focus
- 47 Pages
- Published On: 27-05-2024
Chapter 1: Introduction
Introduction
Sickle cell disease has been reported as one of the foremost genetic diseases in the world. The World Health Organization has thus declared the condition as a priority of public health owing to the detrimental effects that it presents with. The various physical manifestations that the condition presents with are inclusive of pain that is recurrent in nature, strokes, and ulcers of the legs alongside various other ailments. The disease has also been noted to shorten the lifespans of the victims. It has the potential of causing various psychosocial effects such as feelings of isolation, loneliness, poor interpersonal relationships, and stigma as well loss of independence.

The definition of stigma according to the Goffman’s social theory of stigma is a phenomenon where a person is rejected based on the attribute or the behavior that is discredited by the society’ (Ola et al., 2016). In the field of health, stigma has been associated with social discrediting of particular health condition. In the case of SCD, the victims have often reported being stigmatized based on the misunderstandings that the society has had on the diseases besides the races that they come from based on the data that SCD is more prevalent among the minority populations or the marginalized populations of the society.
Background to the Study
The general public lacks education on SCD thus they tend to formulate their own opinions about SCD and these are typically negative. Besides, they have been reported to devalue people suffering from SCD and leading to them experiencing status loss (Martin et al., 2018). Besides, SCD patients result in their pain experiences being discredited by others. They are often accused of not only being weak, but also lazy and always pretending to be ill. The general public treat people with SCD as people experiencing cognitive and physical impairments which make them unable to accomplish their life milestones and goals (Martin et al., 2018). Besides, SCD patients and their caregivers report stigmatizing experiences in their intimate relationships owing to the complications that the condition present with such as priapism, delayed puberty and pain that impairs their sexuality. Various disclosure concerns are associated with individuals revealing their SCD status to others. This emanates from the social stigma that people with SCD experience (Martin et al., 2018). Consequently, SCD patients often opt to keeping their health condition private. In cases when other chose to open up about their status, they often present with regrets (Dyson et al., 2010). Disclosure concerns are caused by factors such as fear of receiving different perceptions and treatment from the general public as well as from close friends and family members. In most occasions SCD patients are pitied and discriminated. Discrimination experiences are reported with SCD patients in places that they work as well as well as in healthcare centres when they reveal their status to the various stakeholders involved in such institutions. Besides, SCD patients often chose not to disclose their status due to the anxiety that is associated with anticipated stigma as well as the attributional ambiguity linked to being unaware of whether the stigma they experience is attributed to the treatment that they receive (Martin et al., 2018). Social stigma associated with SCD impacts greatly on the ability of the patient to receive resources thus this contributes to not only socioeconomic but also racial and medical unfairness.
Looking for further insights on Rising Global Health Burden? Click here.
SCD has thus been a major burden for the caregivers owing to the issues that the literature review identifies. In a study carried out by Ola et al., (2016), the researchers examined the quality of life of caregivers of children with sickle cell disease. From the study, the researchers report that caring for SCD patients poses various demands from the caregivers and these are inclusive of practical, resourceful as well as psychological demands (Ola et al., 2016). It is highly demand to care for individuals with SCD patients owing to both the emotional and practical consequences that it presents with. SCD patients are noted to be dependent on the caregivers for care as well as for monitoring of their health. For instance, the quality of life of SCD patients greatly depends on the wellbeing of their caregivers. The condition has been noted to present with chronic anaemia as well as recurrent acute painful vaso-occlusive crises that usually call for emergency care and management. The burden of caring for SCD patients can be both objective and subjective (Ola et al., 2016). The caregivers always have the duty of administering medication on a daily basis besides promoting behaviours that are aimed at mitigating the pain episodes. Caregivers need to act in appropriate way should the patients present with symptoms by administering the prescribed analgesics and fluids to the patient (Ola et al., 2016). Caring for SCD patients also has psychological effects on the caregivers. They experiencing psychological distress and depression in the act of offering care to SCD patients. Various aspects of life are influenced in addition to their mental health. The perceptions of caregivers have not been sought adequately to determine the burden they experiencing in caring for SCD patients. This research study thus aims to bridge this gap in literature.
Statement of Problem
One of the most prevalent genetic diseases, according to research, is sickle cell disease. As a result, the World Health Organization has designated the condition a public health priority because of its detrimental effects. Among the many physical manifestations of the disease are recurrent pain, strokes, and leg ulcers, to name just a few of the most common. The disease has also been shown to shorten the lives of those who suffer from it. Isolation, loneliness, poor interpersonal relationships, and stigma can all result in a loss of one's sense of self-worth and self-confidence. The disease is associated with stigma which adds to the burden of caring for SCD patients. The issue is thus of great concern and forms the rationale for conducting this research study.
Research Aim
To examine the burden of caring for a child with sickle cell disease, the impact on their quality of life, and the stigma associated with the disease
Research Objectives
- To look at the mental health and emotional impact of caregivers of children living with sickle cell disorder
- To look at the psychological strain that children endure and how they affect their parents' quality of life.
- To address the stigma associated with sickle cell disease.
- To investigate the roles of caregivers in managing pain crises and a child emotional suffering.
Research Questions
- Is the social network of caregivers considerably impacted by chronically debilitating ailments such as sickle cell disease?
- Does the burden of caring for a sickle cell child disrupt their parent well-being?
- Do the pain-management strategies accessible at home aid in the event of a sickle cell crisis from the perspective of a parent?
- How do Beliefs and stigma affect the psychological well-being of children and their informal caregivers?
- What educational resources are available to children with sickle cell Anaemia and their caregivers?
Chapter 2: Literature Review
Introduction
Various studies have examined the psychosocial impacts of stigma on caregivers dealing with patients suffering from SCD. Most of the studies reviewed have reported social stigma from the public as well as family or friends and this has thus contributed to diverse social consequences on the caregivers. SCD patients have been noted to report negative reactions from their family as well as their friends, in some cases, other SCD patients receive such negative reactions from their co-workers, community members and even their peers. This condition has also been a major burden to the caregivers who take care of these patients. This part of the study thus examines what other researchers have done on the topic of study.
Psychological impact of sickle cell disease on caregivers
Some researchers have examined the psychosocial distress that is associated with sickle disease. In 2022, Johnson et al. undertook a study that examined the biopsychosocial factors that have been associated with parenting stress in paediatric sickle cell disease. The researchers noted that caregivers for children suffering from sickle cell diseases face much emotional as well as physical hardship in managing their children diagnosed with sickle cell disease. The study by the researchers thus aimed to examine and identify the biopsychosocial factors that are associated with disease-related parenting stress in children suffering from SCD. The study participants were inclusive of 74 caregiver-youth dyads. From the study, the researchers associated parental stress with an increase in the frequency of child pain as well as increased healthcare utilization. Besides, the researchers also reported an inverse correlation between parenting stress and the mental health as well as the social and emotional function of the caregiver. Besides, the link between child pain frequency and healthcare utilization after the control of parent anxiety as well as the depression that they suffer as a result of caring for children with SCD was also explained by parenting stress. The study thus explained the impact that stress associated with caring for SCD patients has only the emotional and mental wellbeing of the caregivers.
In a different study on the same issue, Madani et al undertook a study in 2018 that examined the quality of life among caregivers of sickle cell disease patients. In their cross sectional study, the researchers examined a total of 164 adults who were caregivers of children that suffered from SCD. They used questionnaires in data collection. From the study, a good percentage of the caregivers were noted to be mothers and were aged from 21-71 years. The results from the research study also noted that most of the participants were from low social class thus they were noted to receive inadequate support and most of their financial needs were unmet. The researchers noted various financial alongside emotional burdens that were faced by the caregivers of children that were suffering from SCD. These thus affected various aspects of their quality of life and were also affected by the personal levels of professional as well as the social attainment. From their study, the researchers were able to recommend that healthcare practitioners should offer specified attention to the quality of life if caregivers especially the impact that their role has on their mental and emotional health as it is a major added burden associated with sickle cell disease. These two studies that are identified from the review of literature note that the mental and emotional health of caregivers is greatly affected by their role in caring for SCD patients.
Stigma associated with sickle cell disease
A study was carried out in Ghana that aimed to examine the stigma that is associated with sickle cell disease in Kumasi (Buser et al., 2021). The researchers noted that stigma is a common trend not only in Ghana but also across the rest of Africa in cases where people suffer from specific kinds of diseases such as SCD. The researchers used in-depth qualitative interviews that entailed the researchers carrying out phenomological study that examined the perception of stigmatization for people that were living with SCD in Kumasi, Ghana (Buser et al., 2021). The participants from the study were mostly female and the findings from the study were categorized into the feelings of social isolation, fear of disclosure as well as bullying about their physique. From the findings by the researchers, stigma is noted to be commonly faced by those suffering from SCD as well as their caregivers. The researchers thus highlighted the need for the development of strategies that are essential in curbing stigma associated with SCD (Buser et al., 2021).
In a different study by Blake et al., the researchers noted that the stress levels of individuals with SCD are influenced by stigma (2017). This is usually common during hospital care when they are stigmatized as drug seeking. Besides, they are stigmatized when they experience delayed care in the emergency department and when their reports are doubted by healthcare providers more concerning pain. Usually, stress present with physiological and psychological effects. The study however notes that it is included in the second domain since the study by Blake et al. based its focus on the psychological nature and effects of stress. One of the major significant predictors of stress that the study notes is the perceived injustice from health care practitioners. Besides, the occurrence of stigma during the lives of SCD patients is tied to various stigmatizing experiences such as being underestimated especially in their academic and physical abilities as well as in losing their jobs based on their SCD status. Blake et al. (2017) added that the daily stressors that people with SCD face includes the illness uncertainty that they experience concerning their pain crises as well as future complications that they may not be aware of. From the study by Blake et al., illness uncertainty and stigma are reported to have a minute correlation (2017).
People tend to be selective when it comes to disclosing their SCD status owing to the stress that is linked to revealing disease and health status (Holloway et al., 2016). From their study, the researchers noted that people suffering from SCD sometimes talk to family or friends about the pain associated with SCD and this has presented with positive psychological adjustment and thus had higher probabilities of seeking care besides having lower awareness of disease stigma as well as being stereotyped. From these findings, the authors tend to argue that it is disadvantageous to fail to disclose status. The study also underscores the significance of strong support in improving not only the psychological but also the physical wellbeing of SCD patients. Stress that comes along with stigmatization affects the mental health of SCD patients. Besides, these individuals are at a risk of suffering from internalized stigma. They experience depressive symptoms that can be inclusive of lacking hope besides losing interest in the activities that they used to engage in on a daily basis. These are positively associated with internalized stigma in individuals that have SCD as noted by Holloway et al., (2016). Other researchers also noted that people with higher experiences of stigma are higher chances of experiencing anxiety as well as depressive symptomatology. Besides, anger, and stress are more likely to be part of their experience relative to SCD patients with reduced stigma rates. SCD patients often report receiving stigma as being drug addicts besides their pain reports being discredited by healthcare professionals. They have also reported having inadequate pain management from healthcare providers. They waited longer in the emergency departments relative to other healthcare practitioners. The pain that SCD patients are often exacerbated with stigma experiences. Besides, reports by studies by Wakefield et al., 2017 and Ola et al., 2016 have indicated that SCD patients experience higher rates of diseases as well as discrimination on the basis of race. In healthcare settings, they usually have higher pain and pain severity, burden as well as the interference with not only daily activities but also their functionality (Wakefield et al., 2017). Ola et al. (2016) also notes that stigma in SCD patients’ impact on their physical wellbeing in the form of self-harm that most of them are reportedly try to engage in. In 2016, Mulchan et al. examined the impacts that stigma due to SCD has on the patient-provider relationships as well as on the care-seeking behaviors of SCD patients. From their study, the researchers reported that SCD patients face race and disease discrimination which affects the health care that they receive. This results in most of them being non-adherent to recommendations that they are given by healthcare providers.
It has also been noted that stigma impacts heavily on the psychological wellbeing of an individual. Harmful effect on the psychological well-being is contributed to by stigmatization of social experiences (Ola et al. 2016). These are inclusive of internalized stigma, anxiety, depression, suicide attempts, suicidal ideation, as well as social isolation. The study describes the various negative effects that stigma has on the mental health as well as the quality of life of people living with SCD. These findings are consistent with those by Wakefiled et al. (2017). According to the findings from the three studies, stigma impacts on the physical function as well as the daily activities besides the general health and social functioning of patients suffering from SCD.
Healthcare inequalities for SCD patients
According to Lee et al., poor access to appropriate healthcare has been reported as a major challenge for people living with SCD (2019). Studies have reported that specialized healthcare providers for SCD are quite scarce in communities of low income as well as in rural communities (Lee et al., 2019). Disparities in receiving care have been reported among the blacks as well as other ethnic minority groups. According to research studies, it has been established that the rate of preventive care is lower among the SCD patients relative to patients that are suffering from other chronic diseases. When counselling and other preventive services are compared, it has been established that more adolescents have received immunization for cystic fibrosis relative to the number of adolescents suffering from SCD (Lee et al., 2019). Besides, majority of children that are suffering from SCD do not get monitored for stroke risk with transcranial Doppler sound. Disparity has also been reported in the access to specialized care by SCD patients. The government has made a number of moves to stop health care inequalities for SCD patients (Lee et al., 2019). First, through the national surveillance system, the government has been able to effectively determine the best allocation of health system resources besides identifying the existing gaps in clinical research. The government has also improved access to care models that have improved access to healthcare (Lee et al., 2019). The issue of shortage of providers has also been addressed alongside various public health implications.
Chapter 3: Methodology
Introduction
"In-depth, open-ended interviews, direct observation, and written documents" are three types of data collection for qualitative findings. A person's thoughts, feelings, experiences, and knowledge can be conveyed through direct quotes in an interview. An observation is a detailed written record of what people are doing in the present moment, as well as what they are thinking and feeling. Survey responses, questionnaires and other publications are all examples of written documentation (Patton, 2002). In situations where data collection is required, surveys are a good option because they allow researchers to collect data from a large number of people and to standardize the data.
Data was collected from caregivers and the following were the research questions:
- Is the social network of caregivers considerably impacted by chronically debilitating ailments such as sickle cell disease?
- Does the burden of caring for a sickle cell child disrupt their parent well-being?
- Do the pain-management strategies accessible at home aid in the event of a sickle cell crisis from the perspective of a parent?
- How do beliefs and stigma affect the psychological well-being of children and their informal caregivers?
- What educational resources are available to children with sickle cell anaemia and their caregivers?
Study population characteristics
The study population comprised a total of 26 participants. From the participants, 12 of them were male while the remaining 14 were female. Besides, from their demographic data, the researcher noted that 5 of the participants were aged between 18-26 years, 6 were aged between 26-36 years, and 7 were aged between 36-55 while the remaining 8 were aged above 55 years. The researcher also sought the ethnicities of the study participants and 10 of them were black British, 4 had mixed ethnicities, 11 were back African while 1 of the participants was of Asian origin. The living as well as the marital status of ten study participants were sought and 3 of the were living with their partners or their spouse, 1 was living with their relative, another 1 was living alone with a child, 2 were divorced, 16 of the study participants were married, 1 was separated while 2 of the study participants were never married before. Considering their religious background, 20 were Christians, 3 were Muslims while other 3 preferred not to disclose their religion. The study participants also had distinct educational qualifications. Of the 26 participants, 1 had no educational qualification, 9 of them were degree holders, 1 was a HNC holder, and other 9 participants were GCSE holders while 6 of the participants were HND holders. All the researchers were presented with the interview questions and given the chance to answer accordingly and their responses are presented in the results section of the research study.
Sampling Strategy
Qualitative research frequently uses people as its primary unit of analysis. The information to be gathered is primarily concerned with the behavior of individuals in a specific setting (Patton, 2002). For the purposes of the present investigation, sampling may include both people and time period strategies. This is critical because people perform or function in various ways during a specific 49 activity (Patton, 2002). Qualitative research focuses on a small number of subjects but examines them in great depth (Patton, 2002). Size of sample depends on research goal and usefulness and credibility of research purpose (Patton, 2002). As a best practice in qualitative research, the researcher should use carefully selected samples to gain a clearer perspective on research topics and questions of interest (Patton, 2002). People who have a lot of information about the topic at hand are selected as participants (Patton, 2002). In order to answer the research questions about the impact of stigma on SCD patients and the burden of caring for SCD patients, a sample of caregivers was selected.
Data collection procedures
Most of the data for qualitative research comes from the field, where the researcher spends a significant amount of time in or around the environment being studied (Castellan, 2010). By allowing the reader to experience the person's "story" through the use of qualitative data, researchers are able to bring their findings to life for the reader (Patton, 2002). The researcher spent time with the caregivers of SCD patients to better understand the burden of caring for SCD patients and the impact of stigma on them. First-hand experience with stigma and burden of caring for SCD patients among 26 study participants was gained through this method. A survey of SCD patients in local care facilities also yielded data.
Data Analysis
The Statistical Package for the Social Sciences (SPSS) was used for data analysis in this study. The software has been developed by IBM and it is widely used to analyse data and make predictions based on specific collections of data. SPSS is easy to learn and enables teachers as well as students to easily derive results with the help of a few commands. The implications of the results are fairly evident and are statistically valid. Using the software, one can conduct a series of studies quickly and effectively. If you are worried about conducting your data analysis on SPSS, here are a few guidelines and an overview of the process. The data collected was first quantified based on the number of respondents for each question. Data was then loaded into an excel file and then imported into SPSS to be analysed. SPSS was then given specific commands depending on what was being analysed. The results were then retrieved from the software given efficiently and accurately, providing researchers a better idea of appropriate future studies and a direction for moving forward. The charts were then analysed and conclusions postulated from the results.
Ethical Considerations
Research must be both useful and ethical in order to be worthwhile (Harwell, 2011). In order to carry out this investigation, we received the green light from the University Review Board. Those who participated in the study were required to provide written consent after being fully informed of the risks involved. To protect the participants' privacy, no data or information that could be used to identify them was collected. Confidentiality was ensured by storing data in a secure location. After the study was completed, participants were assured that all interview notes and tape recordings would be destroyed.
Chapter 4: Results
This section presents that were obtained from the interviews conducted on the study participants. The results are presented according to the research questions that were used as follows. The data that was collected have been statistically tabulated for a better understanding and easier following.
The following were the research questions that the study aimed to answer:
- Is the social network of caregivers considerably impacted by chronically debilitating ailments such as sickle cell disease?
- Does the burden of caring for a sickle cell child disrupt their parent well-being?
- Do the pain-management strategies accessible at home aid in the event of a sickle cell crisis from the perspective of a parent?
- How do beliefs and stigma affect the psychological well-being of children and their informal caregivers?
- What educational resources are available to children with sickle cell anaemia and their caregivers?
Data Presentation
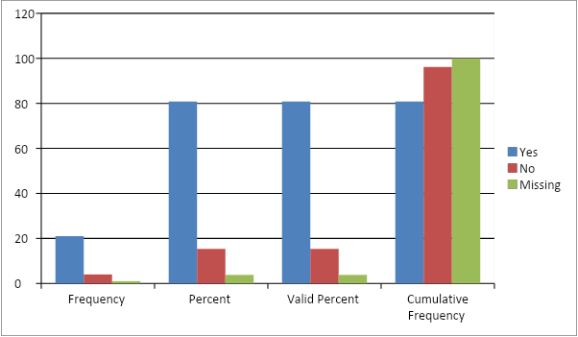
Does caring for SCD patients affect your quality of life?
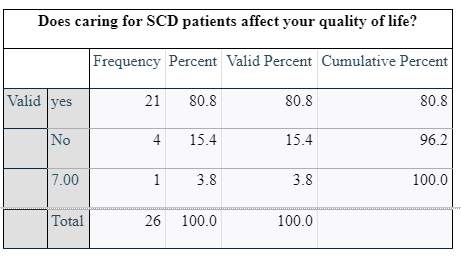
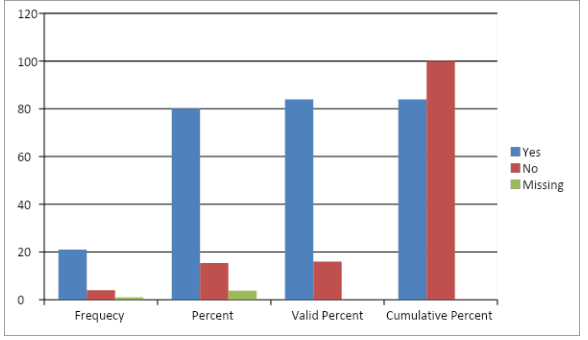
The first interview question sought whether caring for SCD patients affected the quality of life of the care givers. From the responses that were obtained, the researcher noted that 80.8% of the participants responded positively by agreeing that their quality of life was greatly affected by having to care for SCD patients. 15.4 % of the participants however responded negatively by noting that the quality of life was not affected by caring for SCD patients. 3.8% of the participants were however not aware of whether their quality of life was affected by caring for SCD patients. Of the responses, only 3.8% was specific on how their quality of life is affected by caring for SCD patients by noting that it increases stress.
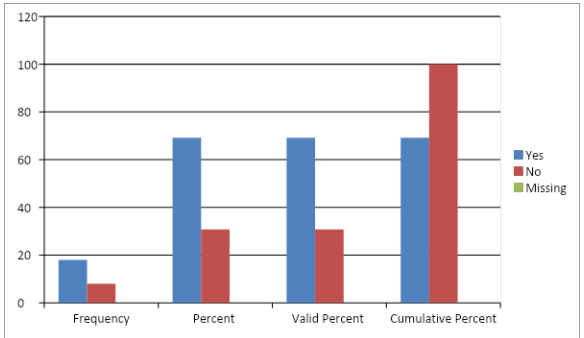
Does the burden of caring for SCD patient affect your well-being?
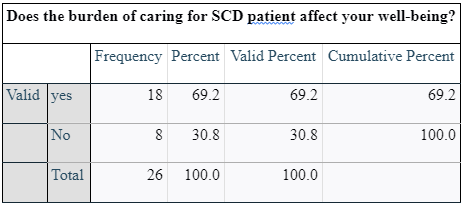
The study participants were also asked whether their well-being is affected with the burden of caring for SCD patents. This question provided an array of responses from the participants. From the data collected, 69.2% of the collected responses indicated that the well-being was affected by the burden of caring for SCD patients. On the other hand, 30.8% of the participants indicated that their well-being was not affected by the burden of caring for SCD patients. Of the 69.2% whose well-being was affected by the burden, 61.1% of them had a different explanation of how they quality of lives were being affected. The noted reasons are as listed below.
- Affect family and everyday life
- Consistent pain and monitoring
- Emotional wellbeing
- Emotionally and physically no peace of mind
- Every part of our lives
- Impacts personal income due to reduced work hours
- Limit one’s ability to socialise
- Pain
- Pain and school attendance
- Recurrent health visits
- The caring part of it and could be tiring
Are there pain-management strategies at home?
The study participants were then asked whether they had access to pain management strategies at home and the following data was obtained.

From the tabulated data, it is notable that 76.9% of the respondents were positive as they agreed that they had pain-management strategies at home while a smaller percentage, that is, 23.1% lacked pain-management strategies at home. Besides, the researcher went on to seek the kind of strategies that they had and out of the 76.9% positive responses, 3.8% of the respondents noted that they had both home and hospital care, another 3.8% noted that they had home treatment while another 3.8% noted that they had medication on manage g the pain though they did not expound on the specific medication that they were using in pain management.
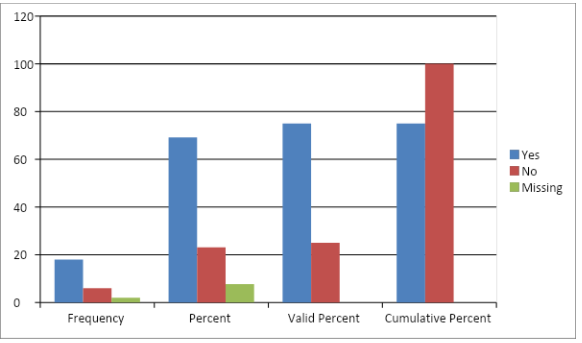
For the participants that that had pain management strategies, they were asked whether the strategies were helpful in the event of sickle-cell crisis. The data that was collected in response to that inquiry was as tabulated:
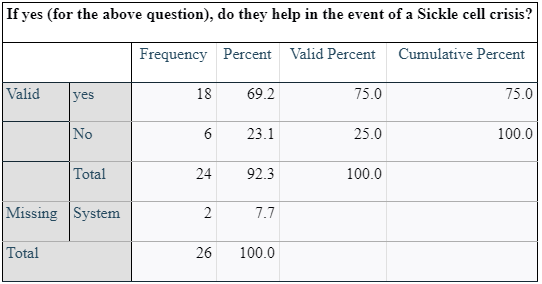
Thus, it is notable that 69.2% of them responded positively while 23.1% of them responded negatively. However, 7.7% of the respondents failed to respond to the question for reasons that they did not explain provide. A small percentage of the positive respondents went further to provide details on how the strategies assisted in time of sickle-cell crisis and the various ways through which the strategies were helpful were as listed.
- It enables to reduce the effects of the crisis
- It is like first aid treatment
- Pain is too much to handle
- Sometimes the pain does not stop
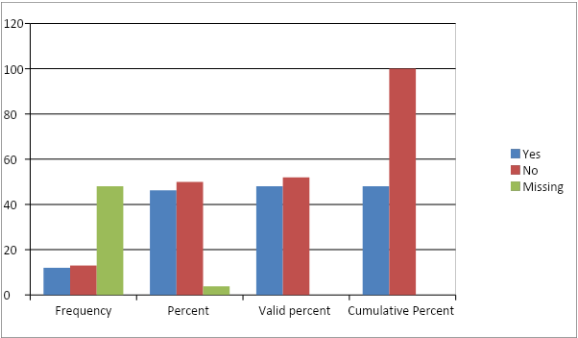
Does your relative of child with sickle cell disease face stigma and discrimination?
The caregivers were asked whether the patients they cared for faced stigma and discrimination and the data collected was as follows.
Looking for further insights on Breast Cancer Prevalence in the UK? Click here.
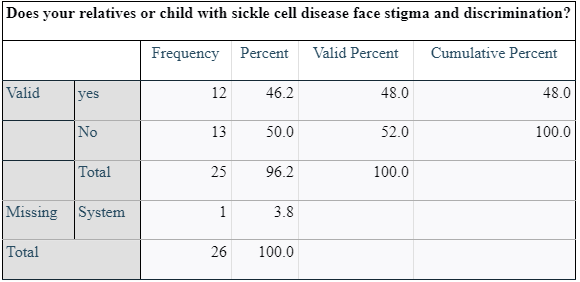
From the data that was collected, 46.2% of the caregivers noted that their patients faced stigma and discrimination while 50% noted that there was no stigma nor discrimination faced by their patients. 3.8% did not respond to the question. The positive respondents further explained how their patients faced stigma and the data collected on the same was as tabulated below.
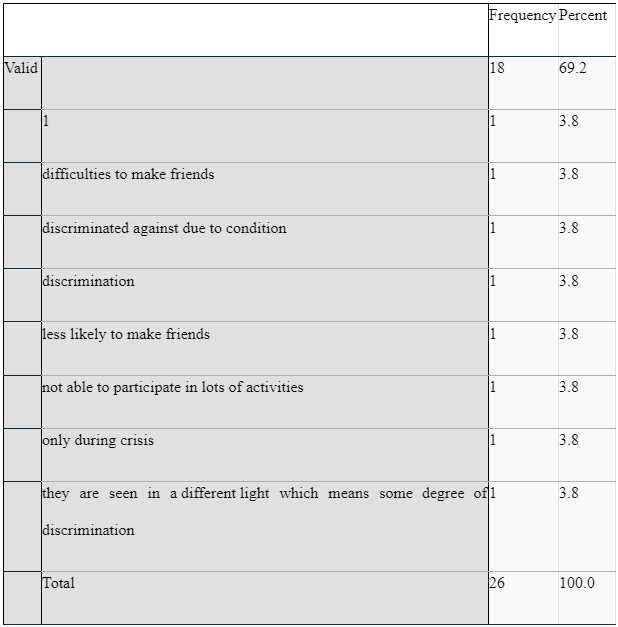
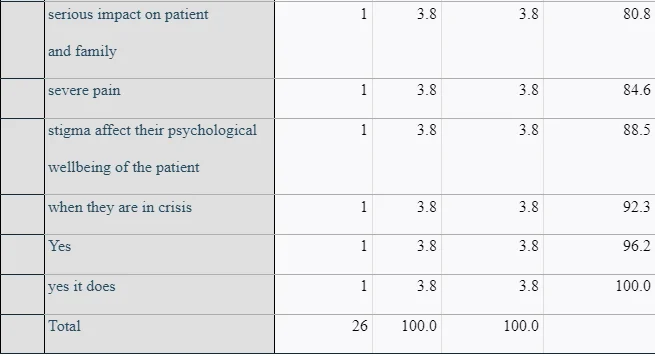
For the respondents that positively responded to the question above, they were asked to explain how stigma affected their psychological health besides the psychological health of the patient that they cared for. Their responses were tabulated as indicated in the table below:
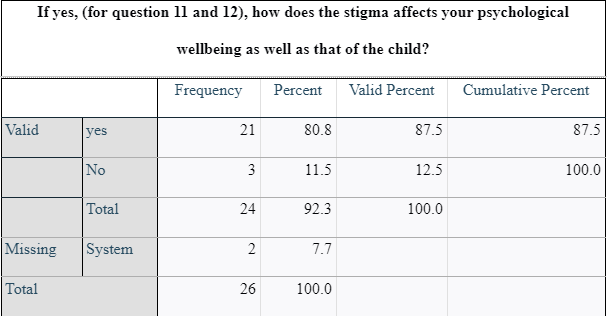
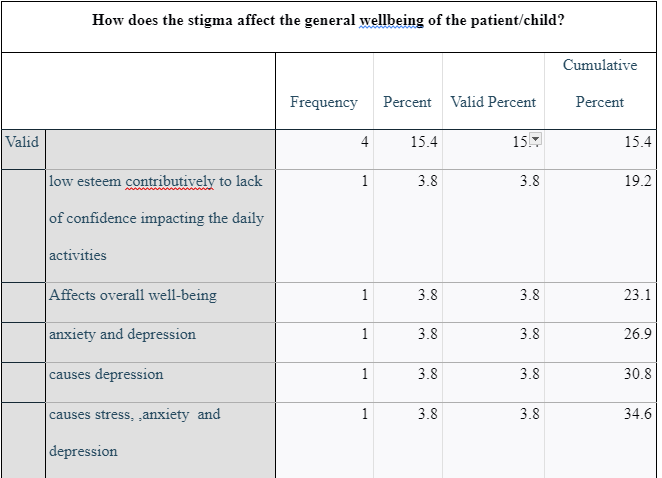
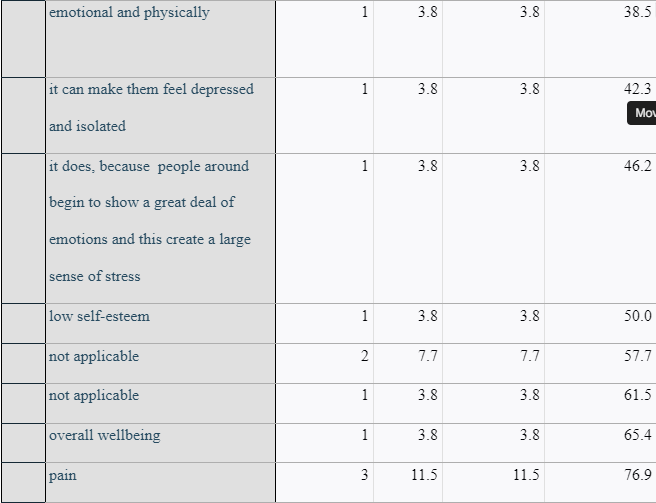
Of the 24 responses, 80.8% was positive while 11.5% was negative. On how stigma affected the wellbeing of the children, the responses were tabulated as follows:
Are there educational resources available to children with sickle cell anaemia?
The study participants were asked whether educational services were available and accessible to the children that suffered from SCD and the data that was collected in response to the question are presented in table form as follows.

From the table that summarised the data, it is notable that 80.8% of the participants had educational services available to the children they cared for while 15.4 % of the participants lacked the same.
The next question that was asked in the interview and the survey was:
Are there resources available as the caregiver?
The responses to the question were as summarised in the table:
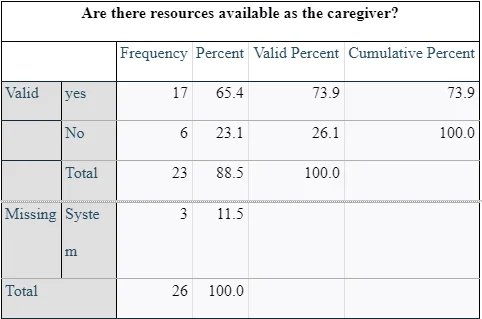
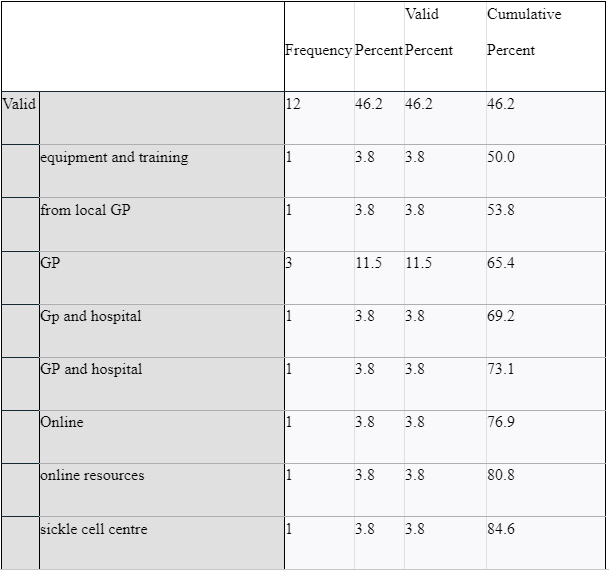
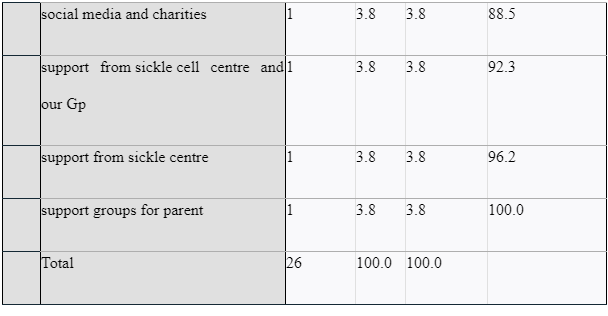
65.4% of the caregivers had resources available to them while 23.1 % of them lacked the resources. Three of the participants that were a representation of 11.5% did not respond to the question. The positive responders went on to provide details on the resources that were available to them and these are similarly tabulated below:
Chapter 5: Discussion
The purpose of this research project was to explore the perceptions of care givers regarding stigma and discrimination that is associated with caring for children suffering from SCD. The first three chapters of this study presented an introduction to the study, it significance, description of the study approach, review of literature relevant to the research study, data production and the data collection methods. The forth chapter of the research study has this presented the data that were collected through the data collection methods that were previously discussed. The fourth chapter contains the interview as well as the survey results.
Discussion
The data that have been gathered from ten research study has allowed the researcher to make a full understanding of the perceptions of caregivers on stigma, discrimination alongside other factors that are associated with caring for children suffering from SCD. The study supports the argument that stigma and discrimination are quite rampant in SCD cases. This section presents a discussion of the collected results while relating the findings to those by other researchers as noted from the review of literature. The results are discussed by answering the research questions through forming various themes from the research questions that have dominated the responses by the study population.
Impact of SCD on social network of caregivers
The study has presented evidence on the diverse impacts of SCD on various life aspects of the caregivers.
The graph below represents a summary of responses concerning impact of being a caregiver for SCD patient on quality of life
The graph below represents a summary of responses concerning impact of being a caregiver for SCD patient on wellbeing
From the interview question on impact of caring for SCD patients on the quality of life, the study noted that from the research participants, the quality of life of 80.8% of the caregivers is affected by caring for SCD patients. Besides, 3.8% of the study participants noted that they are increasingly stressed as a result of caring for SCD patients. These research findings are consistent with the findings by Madani et al. who examined the quality of life among caregivers of sickle cell disease patients (2018). From a cross-sectional study that the researchers undertook involving 63 caregivers, Madani et al. (2018) noted that caring for SCD patients affected the emotions, sleep quality as well as the sexual lives of caregivers. They also noted that caring for SCD patients contributed to lowered job achievement, and poor living conditions as well as their cognitive skills. The findings of this research study on the impact of caring for SCD patients are thus credible ad trustworthy as they are consistent with the findings by other researchers such as Madani et al. (2018) on the issue.
Impact of SCD on well-being of caregiver
This study also investigated the effect that caring for sickle cell disease patients has on the health of the caregivers. The study participants were thus asked to comment on whether caring for SCD patients affected their well-being. From the responses that they gave, it has been noted that 69.2% of them reported their well-being being affected by caring for SCD patients. They went on to explain the various ways through which being caregivers for SCD patients affects their well-being. Less than 50% of the participants had different reasons and they consisted of effects on their family and their daily lives, causing consistent pain that needed monitoring, effects on their emotional well-being, effects on their physical health as well as lack of peace of mind. Another participant noted that affects every part of their life while another one noted that their personal income is affected and reduced as the working hours are greatly reduced.
Pain-management strategies available for SCD patients
This study also aimed to investigate the availability of availability of pain management strategies for SCD patients. The study participants were therefore asked where they had pain management strategies at home.
The graph below represents a summary of responses on importance of pain management strategies in SCD crisis
From the responses gathered by the researcher, the study noted that out of the 26 participants, 76.9% agreed that they had pain management strategies while the remaining 23.1% responded negatively to the question. The positive 76.9% went further to give details on the strategies that were accessible to them and some of the strategies that they noted were inclusive of home and hospital strategies, home treatment for pain as well as medications for pain management. They however failed to give the specific details on the kind of medications that were accessible to them. For the participants that positively responded on the presence of pain management strategies, they were further asked whether the strategies were helpful in the incidences of SCD and different responses were recorded. For instance, 69.2% of them noted that the strategies were helpful in cases of SCD while 23.1% were negative on the importance of the available pain management strategies when it comes to SCD cases. The remaining 7.7% had no information concerning the importance of the strategies in sickle cell disease thus they did not respond to the question. Those who responded positively went on to detail how important the strategies were in cases of sickle cell disease. Amongst the explanations that have been noted from the research study included reduction of the effects of the SCD disease as well as acting as the first aid treatment. Besides, they went on to note that pain management strategies during sickle cell disease crisis helped reduce the pain if is too much to handle besides stopping the pain in certain instances. These findings are equally consistent by what is documented in literature concerning the same. In a study by Okpala & Tawil, the researchers investigated the types of pain management strategies in sickle cell disease (2013). From their study, they noted that pain in SCD can be acute, chronic or sometimes a mixture of the two. They also noted that mediations such as opioids can be used in the treatment of the pain just as is noted in this research study. These study findings are thus valid and accurate.
Effect of stigma on psychological wellbeing of patients and care givers
This study has also investigated the occurrence as well as the effect that stigma and discrimination has on the health of both caregivers as well as the patients. From the study finding, only 46.2% of the respondents noted to have experienced stigma and discrimination while half of them had no incidences or experiences of stigma. These findings are not necessarily a representation of the general population due to the limited study population.
The graph below represents a summary of responses concerning experiences of stigma and discrimination
However, the experience of stigma and discrimination among SCD patients and their caregivers has been largely discussed in literature indicating a consistency of these findings with those by other researchers. For instance, in Kumasi, Ghana, a study was conducted to examine the stigma that sickle cell disease sufferers face (Buser et al., 2021). When it comes to specific diseases like SCD, researchers found that stigma was prevalent in both Ghana and the continent as a whole. The researchers used in-depth qualitative interviews to conduct a phenomological study to examine how people with SCD in Kumasi, Ghana, perceived stigmatization (Buser et al., 2021). More than half of the participants in the study were female, and the findings were categorized into feelings of social isolation, fear of disclosure, and bullying about their physical appearance." This study has also noted that SCD patients that are stigmatized are affected psychologically where by 80.8% of the positive respondents noted that their psychological well-being is affected by stigma and discrimination due to the condition. Stigma is a common problem for people with SCD and their caregivers, according to the findings of the researchers. As a result, the researchers concluded that strategies for reducing the stigma associated with SCD must be developed (Buser et al., 2021). In a separate study by Blake et al., researchers found that stigma has an impact on the stress levels of people with SCD (2017). When they're in the hospital, they're often stigmatized as drug-seekers. Moreover, they are stigmatized when they are delayed in the ER and their reports are questioned by healthcare providers more concerned about pain. Anxiety can cause physical and psychological reactions. It is thus true that stigma is common in SCD cases and it present with diverse effects just has been noted by the studies from literature. This study has also noted that the stigma associated with SCD makes it difficult for the victims to make friends, they cannot take part in most activities, and they are also seen differently.
Educational resources for SCD
The last aim of the study was to investigate the educational resources that are available to children as well as the caregivers with sickle cell disease. In a survey, participants were asked if educational services for children with SCD were available and accessible.
The graph below represents a summary of responses concerning availability of educational resources
Eighty-eight percent of those who took part in the survey said they had educational services for the children they looked after, compared to fifteen percent who did not. A total of 65.4% of caregivers had access to resources, while 23.1% lacked such resources. One-tenth of a percent of the participants failed to answer the question. Those who responded positively went on to describe the resources at their disposal, such as equipment and training from a nearby GP. The educational resources that the study participants listed were inclusive of:
- General practitioner and hospital
- A doctor and hospital
- Online- web-based tools
- Hemoglobinopathies
- Philanthropy and social networking
- From our GP and the sickle cell center
- The sickle center offers its assistance
- Parent-to-parent networks
Studies on this issue are limited thus not much comparison could be made between these findings and those by other researchers. This is thus a gap for future research as there is need to investigate the availability as well as the importance of educational resources not only for children but also adults suffering from sickle-cell disease.
Strengths and limitations
Strengths
- One of the study's benefits is how simple it is to repeat structured interviews because they employ a predetermined set of closed questions that are easy to quantify, making it simple to test for dependability.
- Structured interviews were relatively quick to perform, allowing for a large number of interviews to be conducted in a short period of time.
- The study technique added neutrality to the interviewing process, even when numerous interviewers were participating. Because there was less potential for normal interviewer biases, fair comparisons between candidates were made by constructing a standardized set of questions and assessment techniques.
- Comparing several responses from different people was similarly simple.
Weaknesses
The following were the weakness of the study:
- The interviewee was expected to plan farther ahead of time, which was extremely inconvenient for them at the time.
- The questions required preparation, approval, and testing before they could be approved and put into action.
- The pre-planned set of questions was at danger of being leaked, which may have provided an opportunity for applicants to rig the system.
- It is possible that the questions did not appear to be personal or relevant to each individual applicant.
Recommendations and Conclusion

SCD stigma is a major public health issue. SCD stigma is exacerbated by factors such as disease status, pain and opioid use, racism, disease severity, and socioeconomic status. Institutions, healthcare providers, the general public, and even close family and friends can be the source of stigma. Stigma in SCD has been shown to have a negative impact on individuals with SCD, including affecting social interactions, hindering healthcare interactions, and affecting physiological and psychosocial well-being. Educating themselves and other healthcare professionals about how to interact with and care for people with SCD can help nurses reduce the stigma of the condition. Despite the fact that stigma has the potential to affect social functioning, physiological and psychological well-being, and health outcomes in SCD, it is often overlooked and its effects are undervalued. To reduce the negative impact of stigma on patients, nurses can recognize the effects of stigma and implement interventions to reduce or treat the effects of stigma, such as assessing for mental health needs and addressing challenges related to support.
References
- Adeyemo, T. A., Ojewunmi, O. O., Diaku‐Akinwumi, I. N., Ayinde, O. C., & Akanmu, A. S. (2015). Health related quality of life and perception of stigmatisation in adolescents living with sickle cell disease in Nigeria: A cross sectional study. Pediatric blood & cancer, 62(7), 1245-1251.
- Al Raqaishi, H., Al Qadire, M., Alzaabi, O., & Al Omari, O. (2021). Health-Related Stigma, Social Support, Self-Efficacy, and Self-Care Actions Among Adults With Sickle Cell Disease in Oman. Clinical Nursing Research, 10547738211046731.
- Blake, A., Asnani, V., Leger, R. R., Harris, J., Odesina, V., Hemmings, D. L., ... & Asnani, M. R. (2018). Stigma and illness uncertainty: adding to the burden of sickle cell disease. Hematology, 23(2), 122-130.
- Bulgin, D., Tanabe, P., & Jenerette, C. (2018). Stigma of sickle cell disease: A systematic review. Issues in mental health nursing, 39(8), 675-686.
- Buser, J. M., Bakari, A., Seidu, A. A., Paintsil, V., Osei-Akoto, A., Amoah, R., ... & Moyer, C. A. (2021). Stigma Associated With Sickle Cell Disease in Kumasi, Ghana. Journal of Transcultural Nursing, 32(6), 757-764.
- Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). Thousand Oaks: CA: Sage Publications.
- Derlega, V. J., Janda, L. H., Miranda, J., Chen, I. A., Goodman III, B. M., & Smith, W. (2014). How patients' self-disclosure about sickle cell pain episodes to significant others relates to living with sickle cell disease. Pain Medicine, 15(9), 1496-1507.
- Dyson, S. M., Atkin, K., Culley, L. A., Dyson, S. E., Evans, H., & Rowley, D. T. (2010). Disclosure and sickle cell disorder: a mixed methods study of the young person with sickle cell at school. Social Science & Medicine, 70(12), 2036-2044.
- Ezenwa, M., Yao, Y., Molokie, R., Wang, Z., Suarez, M., Zhao, Z., ... & Wilkie, D. (2016). (157) The association of sickle cell-related stigma with physical and emotional symptoms in patients with sickle cell pain. The Journal of Pain, 17(4), S15.
- Harwell, M. R. (2011). Research design in qualitative/quantitative mixed methods. The Sage Handbook for research in education: Pursuing ideas as the keystone of exemplary Inquiry (Second Edition ed.). Thousand Oaks, CA: Sage Publications.
- Holloway, B. M., McGill, L. S., & Bediako, S. M. (2017). Depressive symptoms and sickle cell pain: The moderating role of internalized stigma. Stigma and health, 2(4), 271.
- Hood, A. M., Crosby, L. E., Hanson, E., Shook, L. M., Lebensburger, J. D., Madan-Swain, A., ... & Trost, Z. (2020). The influence of perceived racial bias and health-related stigma on quality of life among children with sickle cell disease. Ethnicity & Health, 1-14.
- Johnson, Y.L., Woodward, K., Dampier, C., Cohen, L. and Sil, S., 2022. Biopsychosocial Factors Associated with Parenting Stress in Pediatric Sickle Cell Disease. Journal of Clinical Psychology in Medical Settings, pp.1-10.
- Labore, N., Mawn, B., Dixon, J., & Andemariam, B. (2017). Exploring transition to self-management within the culture of sickle cell disease. Journal of Transcultural Nursing, 28(1), 70-78.
- Leger, R. R., Wagner, L. D., & Odesina, V. (2018). Stigma in adults with sickle cell disease and family members: Scale development and pilot study in the USA and Nigeria. International journal of Africa nursing sciences, 9, 23-29.
- Madani, B.M., Al Raddadi, R., Al Jaouni, S., Omer, M. and Al Awa, M.I., 2018. Quality of life among caregivers of sickle cell disease patients: a cross sectional study. Health and quality of life outcomes, 16(1), pp.1-9.
- Martin, S. R., Cohen, L. L., Mougianis, I., Griffin, A., Sil, S., & Dampier, C. (2018). Stigma and pain in adolescents hospitalized for sickle cell vasoocclusive pain episodes. The Clinical Journal of Pain, 34(5), 438-444.
- Mulchan, S. S., Valenzuela, J. M., Crosby, L. E., & Diaz Pow Sang, C. (2016). Applicability of the SMART model of transition readiness for sickle-cell disease. Journal of Pediatric Psychology, 41(5), 543-554.
- Okpala, I., & Tawil, A. (2013). Management of pain in sickle-cell disease. Journal of the Royal Society of Medicine, 95(9), 456–458. https://doi.org/10.1258/jrsm.95.9.456
- Ola, B. A., Yates, S. J., & Dyson, S. M. (2016). Living with sickle cell disease and depression in Lagos, Nigeria: A mixed methods study. Social Science & Medicine, 161, 27-36.
- Patton, M. (2002). Qualitative research & evaluation methods (3rd edition). Thousand Oaks, London: Sage Publications.
- Van den Tweel, X. W., Hatzmann, J., Ensink, E., van der Lee, J. H., Peters, M., Fijnvandraat, K., & Grootenhuis, M. (2008). Quality of life of female caregivers of children with sickle cell disease: a survey. haematologica, 93(4), 588-593.
- Wakefield, E. O., Popp, J. M., Dale, L. P., Santanelli, J. P., Pantaleao, A., & Zempsky, W. T. (2017). Perceived racial bias and health-related stigma among youth with sickle cell disease. Journal of Developmental & Behavioral Pediatrics, 38(2), 129-134.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts