Understanding Stroke Types and Impacts
CHAPTER 1: INTRODUCTION
Stroke is a medical condition which results in the death of the brain cell due to reduced blood flow. Generally, there are three types of stroke condition: Ischaemic stroke and transient ischemic attack (TIA), which are due to lack of blood flow; and haemorrhagic which results due to bleeding (World Stroke Organisation (WSO), 2020). Irrespective of the form, the onset of stroke in an individual is associated with reduced functioning of the brain. As of 2016, around 9.5 million individuals suffered from an ischemic stroke, while 4.1 million suffered from haemorrhagic stroke. Around 80 million individuals across the globe had a clinical history of stroke and were still alive in 2016 (WSO 2016). According to the WSO fact sheet 2016, stroke is the second-largest causative agent or condition for the death of an individual following coronary artery disease and stroke-associated death accounts for 5.5 million. With regards to the form of stroke and the death of the individual, around 4.1 million deaths were associated with haemorrhagic stroke whilst ischemic strokes account for 2.7 million. Around 60% of people currently living who have experienced a stroke are under the age of 70 (WSO 2016). The Stroke Association’s (2018) State of the Nation’s report reveals that in every year, more than 100,000 people experience stroke in the UK. There are over 1.2 million stroke survivors in the UK. In England, one in six people will have a stroke in their lifetime. There are around 32,000 stroke-related deaths in England every year. Stroke is the leading cause of death and disability in the UK. Almost 65% of stroke survivors leave hospital with a disability, and one third of stroke survivors experience depression after having a stroke (PHE & Brine, 2018). The annual budget of the incidence of stroke upon society is estimated to be approximately £26 billion (Stroke.org 2018).
Stroke can result in death, however, it may also result in several disabilities for a person, such as affecting the patient’s social functioning or psychological effects that may affect the ability of the person to perform daily routine work. Stroke is also the leading cause of disability across the globe. One of the significant health complications associated with the condition is post-stroke depression (PSD) (Clarke & Forster, 2015). PSD is a mood disorder characterised by depressive symptoms in the stroke survivor and is similar to the major depressive disorder, however, it differs in context of the frequency of particular symptoms (Gainotti et al., 1999). For instance, individuals suffering from PSD in general present with mood fluctuation, retardation, irritability or apathy while symptoms such as pessimism, anhedonia, suicidal ideation and tendency or attention deficient, are majorly observed in the context of individual suffering from a major depressive disorder. According to a 2014 meta-analysis study, the incidence rate for the PSD was around 31% (Hackett & Pickles, 2014) whilst a narrative review of the research evidence reported the prevalence from 5 to 67% amongst patients suffering from a different form of stroke (Ferro et al., 2009). Despite the clinical condition being frequently observed within the health and social care across the individual suffering from the stroke, there is lack of guidelines for supporting, assessing, treating and preventing PSD (Towfighi et al., 2017). Furthermore, in the daily care and support delivered for the stroke patient, the depressive symptoms remain unrecognised and untreated (Robinson & Jorge, 2016). Biochemical changes in the brain after stroke is one of the reasons stroke victims experience depression (Hackett & Pickles, 2014). Stroke affects mood related chemicals in the brain and obstruct their functioning resulting in the person always remaining in the state of questioning their condition, which ultimately leads to experiencing stress and depression (Clarke & Forster, 2015). Since chemicals in the brain encouraging happiness become affected by stroke, the person may no longer be capable of evolving above from depression. When the brain is injured after stroke, the survivor may find it hard to develop positive feelings and emotions within themselves. (Stroke Association 2012). Some of the clinical features of depression among the stroke survivors may include continuous sadness, anxiety, or empty mood for an extended period, restlessness, irritability, negative thoughts, pessimism, feeling of guilt, a sense of worthlessness or helplessness, loss of interest in hobbies and activities, loss of interest in pleasure including sex, fatigue, decreased social life, memory problems, delayed decision making, difficulty in concentrating, insomnia, sudden change in appetite, and suicidal thoughts (Stroke Association 2012).
Nurses play a vital role in minimising the risks of acquiring depression among stroke survivors (Hendriks et al. 2020). Nurses are the people providing care to the survivors in a different medical institution. Nurses are in an ideal position for the detection of depression in patients after stroke through active listening and applying questionnaires that allow patients to express their feelings and alert nurses to possible depression (Biartmarz, Jónsdóttir, and Hafsteinsdóttir, 2017). Many health professionals may ignore the symptoms of the patient even after repeated complaints, but since nurses offer the closest level of services to the patient and the family, they cannot ignore the symptoms and hence play a crucial role in early recognition of post-stroke depression (Hendriks et al. 2020). A variety of questionnaires such as the NICE Stroke Quality Standard, Geriatric Depression Scale (GDS), Montgomery-Asberg Depression Rating Scale (MADRS) and the Patient Health Questionnaire (PHQ-2 and PHQ-9) can be used for the assessment of depression among stroke patients (Mitchell, 2016). Nurses are able to use these questionnaires to identify depression. However, sometimes these questionnaires may be might not be able to identify depression as it is not always clear that the patient will answer the questions truthfully. Nevertheless, if nurses have established a good relationship with the patient during rehabilitation, the patient may be open about all these subjects to foster recovery from depression. Nurses do not only have a role in recognition of the condition, but they also help in the management of post-stroke depression. Nurses can incorporate different approaches and build-up good therapeutic relations for supporting the patients for their adaptation and readjustment. Nurses offer support in the management through active listening, education, and referral to support services.
The rationale of the study
As mentioned in the prior sections, depression affects approximately one-third of stroke survivors, it sparks interest and increases curiosity to explore the extent of the link between depression and stroke further. Additionally, it is also observed above, that Post Stroke Depression is the most common mental disorder in stroke survivors, therefore, it indicates the presence of two-way link between these two variables. A number of stroke victims suffer from Post Stroke Depression and this reduces their quality of life. To improve quality of life, it is necessary to explore how nurses can help in this matter. As stroke has been linked with psychiatric co-morbidities, researching these elements may help in limiting the occurrence of such factors that decrease quality of life.

The prime focus of the proposed study is to explore and comprehend the role of the nurse in the recognition and management of post-stroke depression. For accomplishing the aim, an objective has been formulated, which is to “Examine the role of nursing-led intervention on identification and resolution of PSD”.
Chapter 2: Methodology PSD
Research can be defined as an in-depth study of a particular issue, problem or concern that uses a mixture of different scientific and statistical methods (Justham, 2006). Researchers provide convincing evidence to a topic or issue, therefore, which is extensively used to prove or disapprove and identify different factors within the nursing field (Aveyard, 2019). Within the nursing field research assists in the development of knowledge and the expansion of the evidence base which informs nursing care. According to Polit and Beck (2017), the general purpose of nursing research is to answer questions or solve problems relevant to nursing. Therefore, this research is trying to answer the question, “What is the role of the nurses in early recognition and management of Post Stroke Depression?”.
The methodology part of research is dedicated to providing information for conducting the research, selecting literature, the method of using it in the research, keywords used and its sources (Igwenagu, 2016). The literature review is an integral part of any research and has a high level of significance in healthcare as well as in nursing research (Rhoades, 2011). The literature provides useful and insightful information to the researcher; however, it is also essential to identify the specific literature relevant to the study (Snyder, 2019).
While conducting research, three methodology paradigms can be followed, these are quantitative, qualitative and mixed methods data (Polit and Beck 2017). Quantitative research is a type of research in which the results are expressed in numerical terms and require statistical modelling (Polit and Beck 2017). Quantitative research can be used to define measurable concepts but does not provide much in-depth information about the concept (Williamson and Johanson, 2018).
Qualitative research is defined as the systematic investigation of the social phenomena in a natural setting, which includes but are not limited to, the perception of individuals towards experiences of their lives, the behaviour of individual or groups, the functioning of an organisation and the influence of interaction on the relationship (Al-Busaidi, 2008). The prime focus of the researcher in qualitative research is the selection of appropriate data collection approach (Teherani et al., 2015). Particularly, a systematic literature review is adopted wherein, relevant and reliable research articles search with the help of different key-terms, followed by the refinement of the search result by using refinement criteria defined (Cooper et. al., 2014). There are advantages of doing qualitative research such as it provides depth and detailed information about the topic, which is being studied, since the responses are not limited as in quantitative analysis, it offers openness to the study participants (Austin & Sutton 2014). It is also recognised as beneficial in identifying people’s individual experiences. Additionally, unlike quantitative research, it can provide reasoning about why the response was given (Moule and Goodman 2014). Qualitative research also has some disadvantages. The collection of qualitative data is more time consuming which limits the number of participants that can be included in the study. Similarly, the outcome of the study cannot be generalised because of very few study participants (Holloway and Galvin 2016). In the case of a lot of varied responses from different study subject, the analysis can become problematic (Holloway and Galvin 2016). Mixed methods are the combination of both quantitative and qualitative methods of research (Holloway and Galvin 2016). It involves the collection and analysis in quantitative form but the interpretation in the qualitative form (Terrell, 2012). A combination of all three research methods are selected to critique and analyse. Primarily, qualitative methods will be utilised, or mixed method used within this literature review.
To answer the research question and fulfil the research objectives under the selected research type and methodology, a search on the chosen topic was conducted using databases and key words. Whilst searching and selecting literature, it was imperative to ensure that the literature answered the research question. After confirmation of the research question and methodology, the process of the literature search was started. During the literature review, primary sources were favoured over the secondary because of the limited chance of bias and higher accountability of the researcher. Articles using quantitative, qualitative and mixed methods have been reviewed in this study.
The literature review began after setting all these terms. Initially Google Scholar was used for searching this literature, which resulted in different databases. Google Scholar is not considered as an academic search engine, but it does have an extensive choice of literature from various publishers and universities (Biswas 2014). The literature search was conducted in different databases. For nursing research, databases of medical and nursing are the most authentic and reliable sources. Firstly, using the Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO host 2020). CINAHL is considered a useful, trusted and reliable database in relation to research within nursing (Moule et.al 2017). Secondly, PsycINFO is used as all research has been peer reviewed, and easily accessible but does not always keep up with current trend (Baker et.al 2015). Finally, this literature review will utilise Cochrane and Nursing journals (PubMed). PubMed is recognised as one of the largest platforms for healthcare research papers and also as it is an international database it can take longer to search due to the huge capacity of the database (Sayers et. al 2018).
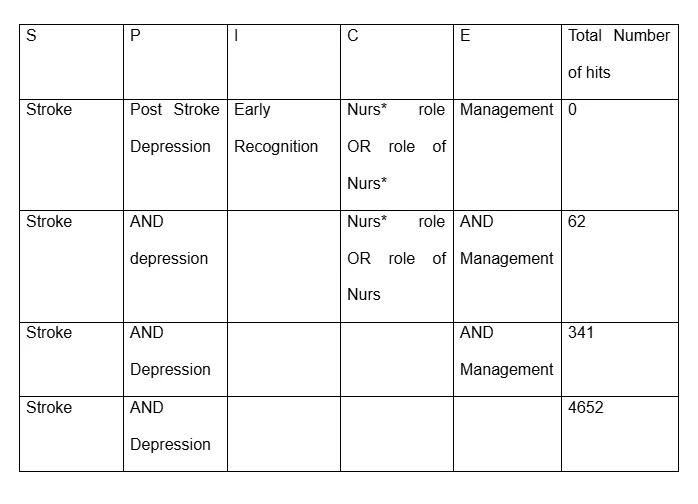
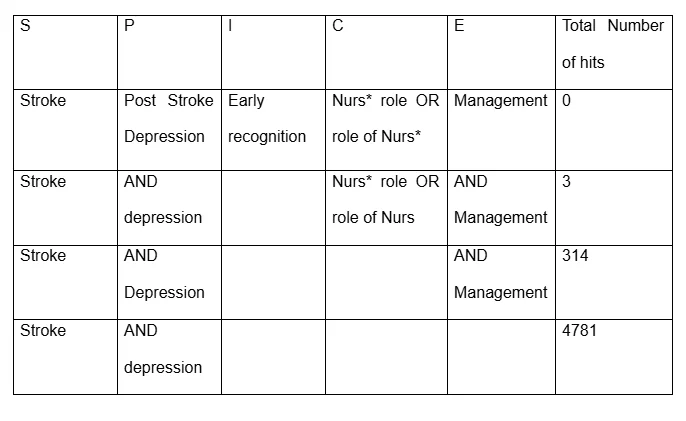
There are various research tools available to search the databases chosen. The acronym SPICE stands for “Settings, Perspective, Intervention, Comparison and Evaluation”. SPICE is a structured and efficient approach identifying relevant evidence only, suitable for evidence-based practice and nursing research (Aveyard 2019). “Problem, Intervention, Comparison and Outcome” = PICO is another comprehensive search tool but can limit the number of recourses available (Methley et.al 2014). “Sample, Phenomena of Interest, Design, Evaluation and Research” = SPIDER is also available and suitable for qualitative literature within health care (Methley et.al 2014). The diagnostic tool chosen for this literature review is SPICE as it is more suitable to evidence-based practice.
Different principle keywords were used for searching the literature, including stroke, depression, management, recognition and the role of nurses. These keywords were used in combination with two Boolean operators “AND” and “OR” to make the research more focused and productive. (Grewal et al., 2016). Truncation is used to enhance a search using a star, dollar or question mark sign, for example, nurs*, instead of nursing, nurse or nurses, (Aveyard 2019).
The initial focus was finding literature about the role of the nurses in early recognition of PSD. Then the focus was shifted on finding how nurses can be of assistance in the management of PSD. After that, the articles that identified the roles of nurses in both the recognition and management were searched for. Plenty of researches have been conducted on this topic. However, it was hard to find the ones conducted, particularly within the last five years. Additionally, the articles that identified the role in both the early recognition and management of PSD were very difficult, and there was very less presence of such articles. However, the selected databases helped the researcher by providing access to thousands of articles related to the topic.

Exclusion and inclusion criteria define the rationale for selecting particular evidence or data within a study or research. The eligibility criteria assist the researcher in refining the research evidence collected and retrieved (Aveyard 2014). Those articles aimed at exploring the role of the nurses in the management of PSD were considered relevant and hence were regarded as the inclusion criteria.

Using the inclusion and exclusion criteria manged to reduce the number of articles as shown below.

The researcher read the abstract of these 45 articles and using the eligibility criteria (Table 4) further reduced the number of articles to super six.

After selecting the relevant articles, the next step was to carry out a critical appraisal. Critical appraisal is a structured process in identifying and evaluating the merits and value of research (Moule et. al 2017). Critiquing involves using a framework, of which there are various different tools available. Aveyard (2019) suggests adopting the use of a critiquing tool as a checklist to evaluate the evidence within a research article and also critical analysis of the research which can enable the author to obtain a greater level of understanding of the articles.

After comparing the frameworks, the researcher chose to use Research Critique framework (Caldwell et al. 2011) to analyse and critique super six articles (table 6), as this framework critiques qualitative, quantitative and mixed methods in a convenient flow chart. This framework primarily considers whether the chosen articles titles have the potential to reflect the content present within the articles. The research framework also includes assessing the credibility of the author. It progresses to analysing the abstract as to whether it provides enough information. The major benefit of this framework is that it considers whether the research papers have used current and relevant literature. No other framework considers this key point which is the main reason for its selection. Finally, ethical considerations are also captured by the framework in relation to the chosen research papers. A table formed to identify similar themes within the six articles, while reading each article individually and in more depth. The table below identifies various themes within the six articles.
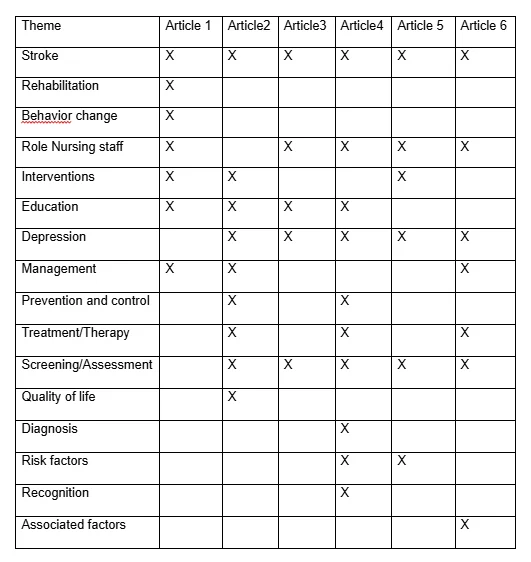
Three main themes were extracted from the contents of the 6 articles which are:
Role of nurses in management of Post Stroke Depression
Various screening tools and assessments to recognise Depression.
Treatment, therapy and management of Post Stroke Depression
Chapter 3: Literature review:
Theme 1 : Role of Nurses in Management of Post Stroke Depression
This chapter offers information about the significant role of the nurses in the management of post-stroke depression. Nurses play an equally remarkable role in the management of post-stroke depression. Nurses are known to build good therapeutic relationships with patients. They can use different approaches to support the adaptation and readjustment of the patient. Approximately one-third of the stroke survivors are affecting depression (Towfighi et al. 2016). The brain damage after a stroke leaves patient with unique physical and mental dysfunctions with which people cannot cope properly and hence develop depression. Depression after stroke generally follows a chronic course and is related to a variety of adverse health outcomes, including increased disability, morbidity and mortality. PSD occurs less than two weeks after a stroke, while late-onset PSD occurs more than two weeks after a stroke (Zhao et al. 2018). Most of the stroke patients rehabilitated in hospitals where nurses provide all necessary care services. Since almost one-third of the stroke patients develop depression, this is a highly prevalent problem. Nurses are working very close to the patients due to the range of services they provide to patients. Nurses are in an ideal position to investigate depression in stroke survivors by active listening and asking open-ended questions that enable patients to express their feelings and alert nurses to possible depression (Mitchell, 2016). Based on the guidelines set by National Institute of Care and Excellence (NICE), nurse is obliged to comply with the Standard and Codes of Practices while managing health needs of the patients with Post Stroke Depression (PSD) [NICE, 2020]. In this context, nurse need to respect the values, decisions, and preferences of patients suffering from PSD. As argued by Towfighi et al. (2017) sometimes nurse face ethical dilemmas while listening to the demand and interest of patient with PSD as the demand in most of the times is irrelevant to the health condition and of patients which can enhance health risk. According to the guidelines set by NMC (National Midwifery Council), during management and treatment of patient with PSD, nurses need to listening to the decisions, problems and opinion of patients raging theft own health management, that assist nurse to understand the actual mental and physical health needs of the patients [NMC, 2020]. In addition to this, one of the most important strategies that every nurse would apply during management of patient with PSD is forming effective communication with patients and their family members. As mentioned by Karamchandani et al. (2015), in management of patients of PSD, nurse ned to make both the verbal and nonverbal communication with patients and family, embers. Through developing clear communication with patients and that family members, nurse can collect important information regarding patient’s mental health such as pre-medical history of the patients, reason behuing the stroke, behavioural changes in patients, preferences, interest, hobby and attitudes (Van Dijk et al. 2018). Through developing effective communication with family members of patients, nurse can understand the actual psychology and attitude of patients with PSD which allow nurse to manage mental and physical health needs of patients. In addition to this, during management of Post Stroke Depression, nurse needs to maintain the clear as well as transparent information delivery system in workplace, which assist nurse, healthcare staffs and health professionals to transfer as well as receive important information regarding the current health condition, current depressive symptoms, behavioural changes and psychological needs of patients. As argued by Karamchandani et al. (2015), sometimes only transparent information delivery system in care homes is not sufficient for management of PSD patient, rather nurse and health care staffs need to focus on eliminating chances of any conflict or misinterpretation of information which can interfere with integrity as well as competence of nurse in management of PSD patients. Under the guidelines set by NICE, while it comes to management of PSD patients, nurse and health professionals need to focus on creating positive and supportive environment surrounding the patients in terms of reduce the level and intensity of depression in them (Harrison et al. 2017). Here nurses would ensure that, patient with PSD has been provided with a safe and secure environment in which her or she is protected from any kind of abuse, harassment, discrimination, molestation and bullying. During management of PSD patients, nurse will conduct polite and friendly approach towards patients which in terms of making the patient ready to share their thoughts, decisions, issues, preferences and opinion with nurses (Karamchandani et al. 2015). In addition to this, nurses need to involve patients with PSD into different intellectual activities that enhance self-confidence in them by reducing the level of mental distress and depression. Nurse always assure that, patient’s decision, issues and preferences are prioritised in management of Post Stroke Depression in which patients are provided relevant care and treatment methods that not only associated with their mental healing but also associated with their emotional and physical healing. In the context Loft et al. (2019) argued that, in case of management of patients with PSD, it is not always possible for nurses to prioritise interest and preferences of patients as it can interfere with treatment process and integrity of health professionals. In this context, nurses can use effective therapies such as Cognitive Behaviour Therapy (CBT), Compassion Focused Therapy (CFT) and Counselling that assist nurse to promote the overall mental and emotional wellbeing in patients.
For conducting proper management of patients with PSD, nurses need to assures that all the mental and physical health needs of patients are assessed by healthcare staffs and professional in effective manner (Towfighi et al. 2017). Nurse also assure that, patients with PSD is provided with suitable medications which are important for improving their overall psychological condition and reducing their depressive symptoms. In addition to this, nurse play important roles in developing inner strength, cognitive skills and interpersonal skills of patients with PSD that are associated with reducing depressive behaviour in patients. Here nurse would assist patients to be involved into intellectual activities such as gardening, playing intellectual games and doing regular activities which are associated with improving the interpersonal skill and self-confidence of patients (Karamchandani et al. 2015). In addition to this, nurses also listen to the needs, issues and preferences of patients while managing their needs rather than establishing only own view points. During engagement of PSD, patients nurse plays important roles in involving patients into their own recovery which is associated with reducing depressive symptoms in patients with PSD (Tulek et al. 2018). Here nurse assist patients to be involved in taking decisions and share issues regarding their management and treatment process which enhance the transparency and clarification in the overall indication between nurse and patients. In addition to this nurse also ensure that the overall management and treatment process that are implement into practice are able to reduce the intensity and severity of depression on patient’s thoughts, decisions, and opinions (Van Dijk et al. 2018). Nurses also play important roles in improving health literacy of patient as well as of the family members which is important for management and recovery of patients. Nurse can conduct training and self-assessment program for the patients with PSD which can allow patients to asses their needs, self-confidences, behavioural changes throughout treatment and management process. In addition to this, training and development of patients with PSD can asst nurse to train patients about their self-management, self-protection and actualisation of positive thoughts, decision as well as perception, which improves the overall mental and emotional wellbeing of patient by reducing the intensity of depressive symptoms.
Theme 2: Various screening tools and assessments to recognise Depression.
Early recognition, prevention and treatment of PSD are vital to the recovery and prognosis of stroke survivors (Zhao et al. 2018). Nursing staff and family caregivers play a vital role in the detection of depression among stroke patients (Zhao et al. 2018). PSD aggravates the burden of physical, psychological and social disability after a stroke, and hinders patient’s participation in rehabilitation. Thus, the early detection of PSD is highly essential for optimized patient recovery. The NICE Stroke Quality Standard (2016) suggests, “All patients after stroke need to be screened for depression within six weeks of diagnosis, by using a validated tool.” Formal screening of depression can be time-consuming, but nurses may consider asking patients if they have had often been bothered by feeling down, depressed, or hopeless or if they have had little interest or pleasure in doing things (Karamchandani et al., 2015). Nurses are known to have a unique screening role for post-stroke depression; also, nurses experienced a hard time in the assessment of the psychological status because of lack of knowledge, skills and training. While it comes to discuss the screening as well as assessing of PSD, it is important to discuss the purpose behind conducting these tools or assessment processes. As mentioned by Van Dijk et al. (2018), health professional need to select relevant screening and assessment tools in case of PSD to make effective clinical intervention of the mental, physical and emotional health of patient who had gone through the stroke. Based on the guidelines and standard of care set by National Institution of Care and Excellence [NICE], had mentioned that in terms of dealing with a patient with PSD, health professionals need to use relevant screening and assessment tools which will assist them to analyse the symptomology, pathophysiology and pharmacological aspects associated with the PSD condition [NICE, 2010]. There are different assessment and screening tools for PSD, which as follows:
Clinical Assessment tools:
Self-Administered mood scale: Beck depression inventory and PHQ-9 [Patient Health Questionares-9] questions
Psychology or Therapy tools:
CBT tool (Cognitive behavioural therapy tool)
CFT tool (Compassion Focused Therapy Tool)
Others:
Self-report screening tools
Geriatric depression tools (GRS)
Visual Analogue Mood Scale (VAMS)
Aphasic Depression Rating Scale (ADRS)
Clinical assessment tools:
The timely detection of PSD is affected by the shorter length of hospital stay resulting in more cases and increased severity of PSD. Nurses can use different screening tools for recognition of PSD.
PHQ-9, known as the patient health questionnaire, is a questionnaire-based screening tool. It can be used to diagnose the major depressive syndrome. It is a nine-item depression scale of the patient health questionnaire. It is regarded as one of the most validated tools in mental health and can be a powerful tool to assist clinicians while diagnosing depression and monitoring treatment response. PHQ-9 has also been used several studies for the screening of Post Stroke Depression. There are different advantages of the PHQ-9 like shorter than other depression rating scales, can be self-administered or also administered by a health professional or nurses, provides an assessment of symptom severity, is well validated and documented in a variety of populations and also can be used in a wide variety of population according to the age. Research article entitled, “Early Depression Screening is Feasible in Hospitalized Stroke Patients” (Karamchandani et al., 2015) has used a modified Patient Health Questionnaire (PHQ-9) to assess the post-stroke depression. The main reason for modification was that the study needed to detect depressive symptom since the time of hospitalization rather than in the preceding two weeks. The modified PHQ-9 was named as MPHQ-9, which was self- administered. The scores ranged from 0-no depression to 27- severe depression (Karamchandani et al., 2015). The corresponding actions were taken according to the score after the study. Another important depression assessment and screening tool is Beck Depression Inventory (BDI). BDI is highly validated and well-reliable screening tool that consist of 21 items of questions (Zhao et al. 2018). Questions are designed in such a manner which assists health professionals to determine as well as measure the symptomology of PSD, characteristics, attitudes and behavioural changes in patient who had gone through stroke. This tool is the self-rating inventory, that assist patients to rate their feelings, attitudes characteristic features, behaviour and experiences (Karamchandani et al. 2015). Although BDI is reliable and effective screening tool in measuring depression, thee are many criticisms regarding its effectiveness and implementation in all types of patients with PSD. As mentioned by Loft et al. (2019), BDI is north an effective assessment tool in older as well as disabled patients, as the patient are unable to evaluate as well as understand the own feeling, characters and experience, that makes it difficult for patients to rate own attitudes or features. On the other hand, in case of patients with dementia and other meal disorders, ether is huge mood swing and behavioural challenges in patients that make it difficult for these patients to rate their behaviour and feelings they have after the stroke. In this context Van Dijk et al. (2018) argued that, although BDI can nit be used in some special cases such as in case of the disabled patient or older patients, the overall screening method by using the BDI items assists health professional to measure the severity, intensity and depth as well as frequency of depression in a PSD patient. Among all the 21 question each question is made to define as well as evaluate a definite symptom associated with PSD. Through analysing the rating made by the patients, health professional compares them accordingly in terms of understating that how severe is the impact pf Post Stroke Depression on mental, emotional and spiritual wellbeing of patients.
Phycology or Therapy tools:
CBT tool is one of the most commonly used psychology or therapy tool which assists health professional to use different techniques associated with this BDT tool to record the intensity and severity of depression on mental and physical health of the patient suffering from PSD (Towfighi et al. 2017). Here health professionals can use online worksheet such as Activity diary, activity planning log book, activity selection, assertive communication logbook, assertive responses worksheet and avoidance hierarchy. Through conducting this tool, health professional determines current cognitive behavioural condition of patients with PSD and its connection with the depression. As argued by Karamchandani et al. (2015), by using CBT tools the health professionals are able to determine how the thoughts, intelligence and decision-making process are affected by depression after the stroke, but they are unable to measure correct intensity and depth of depression in patient in post-stroke condition. Although there are many criticisms reading using CBT tool, it is acknowledged that, CBT screening process is not only associated with determining intensity and severity of depressive thoughts as well as poor decision-making process in patients, but also the tool is associated with improving cognitive skills by developing positive ideas, thoughts and experiences in patients. Another important assessment tool for PSD is CFT (Compassion focused Therapy), that focuses on assessing as well as measuring emotional and spiritual distress of a person due PSD condition (Cassidy et al. 2018). This assessment tool is associated with emotional and spiritual healing of PSD patient will making them compassionate toward themselves as well as towards the other people. As mentioned by Van Dijk et al. (2018), this tool assist health [professionals to assess the impact of PSD on emotional and spiritual wellbeing of patients. In addition to this, health professional use activity log book, in terms of rating the severity and intensity of the spiritual and emotional distress of the patient with PDS, which determines the actual cognitive condition of patients.
Other tools
Geriatric depression tool (GRS) is one of the reliable and valid assessment and screening process that consist of 15 questions regarding the feelings, depressive thoughts, negative experiences, sadness, assumption and perception of patients suffering from PSD (Karamchandani et al. 2015). This is self-rating assessment tool that assists health professionals to measure as well as determine the severity of depressive feeling, bereavements, negative assumption and perception. In the context Van Dijk et al. (2018) argued that, HGRS is not all time effective for the health professional to get the actual measurement of severity of depression in patients suffering from PSD, as it is possible that many of the older and disabled patients cannot use the correct ratings in each answer, that enhances the chances of error in the results. In this context, there is another important screening and assessment tool that can be used by health professional in primary care while determining the severity of depressive condition in PSD patient, the Visual Analogue Mood Scale (VAMS). This is one of the highly preferred and recommended assessment tools that can measure eight different moods in patients with PSD such as confused, tired, angry, sad, afraid, energetic, tensed and happy (Zhao et al. 2018). This scale has 10 rating options (1 to 10) for each mood status, which allow respondents to give ratings based on the intensity of mood status. As mentioned by Atique-Ur-Rehman and Neill (2019), VAMS is effective in measuring the severity of deterioration of each mood condition in patient with PSD. In primary health car process, the VMAS mood scales are high effective in measuring impact on PSD on feelings, assumption, perception, experiences and decision-making process of the patients. Another important tools, in assessing depressive condition in PSD patients is, Aphasic Depression Rating Scale (ADRS), which is generally used in determining depression in Post Stroke patients who has aphasia (language impairment) (Rosas et al. 2019). There are many criticisms regarding using ADRS as screening tool of assessment of depression in PSD patients. In this context Towfighi et al. (2017) stated that, ADRS is not relevant screening and assessment tool in case of all types of post -stroke patients with PSD, rather the tool can only be successfully used in post-stroke patients having aphasia. From all overall discussion, it can be stated that there are many screening and assessment tools in determine as well as measuring severity of depression in patients with PSD. Now implementation of any of the above-mentioned tools would depend of types of depression, health needs and current mental, physical and emotional health of the patients. In addition to this. Health professional also need to evaluate the ratings and scales by using order evidences and probability value, to get the accurate measurement of intensity of depression in PSD patients.
Theme 3: Treatment, therapy and management of Post Stroke Depression
Individuals with PSD are at a higher risk for suboptimal recovery, recurrent vascular events, reduced quality of life, and mortality. Even though Post Stroke Depression is highly prevalent, there still exists uncertainty regarding the risk factors and optimal strategies for prevention and treatment (Towfighi et al., 2017). Post-stroke depression is not a different type of depression; it is just that the patients of stroke are involved. But the severity of the symptoms is higher among stroke patients with PSD. While it comes to discuss the treatment of individual with PSD, it is important to discuss the types of treatments in healing the depressing condition of the patient (Towfighi et al. 2017). Evidence-based report suggested that, as no definite pathophysiology and risk factors are determined in case of PSD, it is stated here is no definite treatment process for mental health condition, today’s health professionals and therapist use antidepressants and psychotherapies that can heal emotional and mental distress in patients with PSD. Evidence-based studies have mentioned that the are two different treatment and management process for PSD, the pharmaceutical treatment and non-pharmaceutical treatment process.
Pharmacological treatment process:
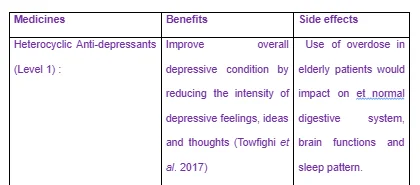
While using pharmaceutical treatment process for PSD patients, the health professional prescribes antidepressant medicines that can reduce the severity and intensity of depressive thoughts and feeling in the PSD patients (Hussein et al. 2019). Drug therapy helps in improving neurological outcomes and long-term prognosis. The drug therapy is not a sole contributor if there’s no good hospital-patient relationship. Nurses along with other health care providers, play a critical role in improving this. The PSD patients should be on antidepressants as soon as they are diagnosed with depression. Whereas, the choice of the drugs used for the treatment is based on the symptoms of the patients and the side effects for the elderly. The clinicians should observe the response of the patients to the therapy in order to monitor their healing process. If the medicine doesn’t seem to be working effectively, then changes should be made on the medication. Sometimes the doses of the medicine are not suitable for the patients and they might get a panic attack, which should be monitored carefully before prescribing.
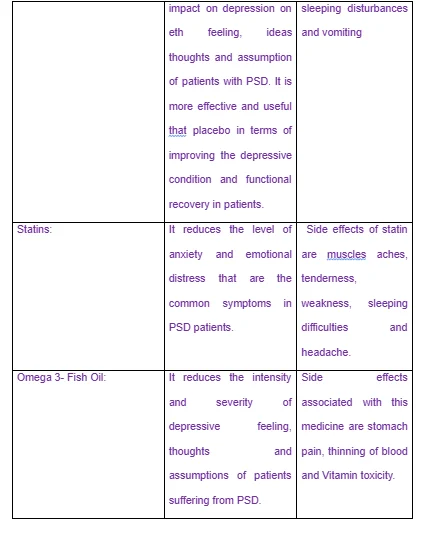
Different medicines are used in this treatment process which are as follows:
Medicines used in treatment of PSD patients and their benefits

Non pharmacological treatment process of PSD:
In case of this treatment process, health professionals and therapist use effective therapeutic tools that are beneficial to reduce depressive symptom in individual with PSD. During the treatment and management of individual with PSD, one of the most common as well as effective therapeutic tools is Cognitive Behavioral Therapy (CBT). As mentioned by Karamchandani et al. (2015), CBT is well-organized psychotherapeutic approach which is associated with improving the psychology, emotion and decision-making process in human mind, in case of treating depression in individuals with PSD, CBT is highly effective which allows the mental health professionals as well as therapist to check the current cognitive behavior and skills in patients with PSD and how the behavioral is connected to increasing level of depression after stroke in that individual. As argued by Van Dijk et al. (2018), sometimes CBT is effective only in determining connection between cognitive distress and depression condition of patients with PDSD, rather than developing effective strategies in dealing depressive condition. CBT consists of three major process such as initial phase, middle phase and final phase. In the initial phase, therapists evaluate and analyze current mental and psychological condition of patients with PSD in terms of measuring the intensity as well as severity of the depressive thoughts and ideas in the patients (Zhao et al. 2018). On the other hand, in middle phase the, therapist and mental health practitioners can set behavioral and cognitive strategies that are relevant with the current mental and psychological condition of patients. In final phase, the therapists implement these strategies by using proper clinical intervention into practice that can reduce the depressive symptoms in individual with PSD.
Another important therapeutic treatment that many health professionals and therapist use in current clinical field is Compassion Focused Therapy (CFT). This therapy is associated with emotional and psychological healing of patients suffering from PSD. As mentioned by Valiengo et al. (2017), CFT is proved to be highly effective in treatment of depression in patients with PSD, that prioritizes the development of positive thoughts, ideas and perception in patients which improves their decision-making skills nod problem-solving process. By using this therapeutic tool, mental health practitioners can determine how depression in patients with PSD can pose negative impact on their ideas, ideas and thoughts. This process is highly effective in spiritual development of patient with PSD in which social, infection, family support and connection with external world is introduces into this therapy in terms of healing emotional and spiritual distress in patient with PSD. Another important therapy used by mental health professional as well as therapists is Mindfulness-Based Cognitive Therapy (MBCT) (Loft et al. (2019). In this therapeutic process, mental health professionals as well as therapists analyse the impact of Post Stroke Depression on mental processes of patients such as their decisions, analysing skill, judgemental skill, reasoning, assumption, perception and ideas. Through evaluating the mental processes in PSD patients this tool assists mental health professional to develop effective clinical setting that would reduce the depressive symptom in PSD patients. As argued by Van Dijk et al. (2018), in case of dealing with PSD patients who have mental disorder, it is difficult to cure the overall mental and psychological condition of patients by only prioritising the mental and emotional healing, rather than mental health professionals need to focus on promoting physical and spiritual wellbeing which can improve the overall decision-making, thoughts, behaviour and activities of patients. Another important therapy or tools is counselling which is associated with analysing the current mental processes human being. As mentioned by Towfighi et al. (2017), counselling can be used in reducing depressive symptoms in patients with PSD, in which the psychiatrists set effective strategies in involving patient to his or her own mental and physical recovery, such as convincing patients to share their decisions, preferences issues with psychiatrist so that the psychiatrist can understand what’s wring with them. From the above-mentioned discussion, it can be stated that, although pathophysiology and risk factors of PSD is obscure and unknown, there are effective therapies, assessment tools and anti-depressants which can reduce the depressive symptoms in patients with PSD. In addition to this, mental health professionals, psychiatrist and therapists need to understand the overall mental and physical health needs of patients with PSD before using as well as implementing any of treatment processes in terms of promoting psychological, spiritual, emotional and physical wellbeing in them.

Chapter 4: Discussion
This section has discussed the findings of the secondary articles that are selected by the researcher. Here the researcher not only discussed the information from each article thar has assisted the researcher to conduct the research in effective manner to meet the research objectives, but also in this section researcher has critically analyzed the limitations as well as drawbacks of each article in terms of providing relevant information for this study.
Towfighi et al. (2017) have mentioned in their article that, depression is most common mental health condition in patients that affects one third of the stroke survivors. Based on the viewpoint of this article, the actual cause of PSD is still obscure and unknown to the health professionals despite wide ranges of research have been conducted on this topic. evidences based report have suggested that there are many factors that are associated with PSD such as psychosocial, sociological, economic and psychological factors which pose adverse impact on overall connection between the body and mind of stroke survivors. In this context Karamchandani et al. (2015) argued that although there are social, economic and cultural factors associated with occurring PSD, evidences-based studies have mentioned the strong connection of genes and heredity with PSD in many patients. whatever the reason behind occurring of PSD, it is proved that, the stroke survivors need to be provided with proper support and care by nurses and health professions to meet critical needs of patients. Van Dijk et al. (2018) has mentioned in their article that, nurses are the foundation of a healthcare system who play important roles in proper care and management of Post Stroke Depression. Based on the discussion of this article it can be stated that, nurses need motivation and support from higher healthcare officials in terms of involving them to develop highly effective nurse-led intervention of PSD which not only assist the patients with PSD to recover the metal as well as physical health condition, but also assist patients to improve cognitive strength, decision making ability and problem solving skills. in this context, there are many evidence-based report which argued that, for proper management of PSD it is not sufficient for healthcare authority to develop the nurse-led intervention process , rather healthcare management team needs to conduct proper educational and training program for nurse to make consistent improvement of their professional standard which will assist the nurse to brings about innovating strategies in the intervention process while managing the neds of PSD patient.
Evidence-based studies have stated, early screening in one of the most feasible process that can be used by nurses in modern clinical field, in making innovative management and better treatment of patient with PSD (Karamchandani et al. 2015). There are many criticism with this statement, in which many health professionals think that , as the reason behind PSD is still unknown, screening is not always effective in managing the mental and physical health condition of PSD patients, rather they have mentioned their preferences of psychotherapy, Cognitive development therapy (CDT) and counselling that can be used by the community nurse to improve the overall mental condition of PSD patients.
According to Zhao et al. (2018), clinical practice guidelines of post-stroke depression prioritises the determination of risk factors associated with PSD such as social biological, economic, psychological and mental factors and early recognitional treatment and prevention of PSD condition by Nurse. recent studies have mentioned the importance of conducting innovative psychotherapies that will improve the psychological condition of patients with PSD, as depression is strongly associated with psychological distress. In this context Loft et al. (2019.) argued that, for managing the need of PSD patients and promoting their health as well as wellbeing it is not sufficient to improve their mental condition, rather the health care authority needs to conduct proper educational programme and self-assessment programme for nurses which will assist them to bring about innovation in overall clinical intervention and psychotherapies in terms of meeting changing health needs of PSD patients.
Hospital nursing unit plays an important role in the identification and recovery of the PSD patients who have a specific set of needs for the cure. A nurse's level of understanding about the disorder can have an impactful influence on diagnosing the development and prognosis of PSD. Appropriate nursing care should be based on the outcomes of the nursing assessment which includes physical, mental status and associated risk factors. The general objective for the management of PSD incorporating the nurse’s role in the plan should consist of a comfortable environment, appropriate personal care (including nutrition supplements), and a relaxing sleeping environment to assure adequate rest (Zhao et al., 2018).
Several of the studies reviewed showcased that assessing depression in the acute phase bears high importance. If not identified on time, the stroke survivors with depression have increased chances of having continued depression, poorer outcomes, and high functional dependence. The outcome can be as severe as death, as well. More qualitative studies are needed for an in-depth understanding of the post-stroke depression. The use of a variety of mood scales can help achieve the ideal measuring scale that can be implemented for measuring the depression among stroke patients explaining all their constraints. In most of the studies, it was found that the gold standard for the measurement of depression in both the acute and post-stroke phase in absent. One of the critical issues that most of the researches stated for the assessment of depressive disorder is the absence of qualification in nurses due to the lack of training. Some of the researches even emphasised the assessment or management to be in the presence of guidance from a psychiatric or a psychologist. A need for continued empirical research on the profile and patterns of PSD explaining the individuality of the cases of PSD was quoted necessary by almost all the literatures to reduce the mortality. All the literatures reviewed have their own purpose for conducting the research, some focused on the real need of nurses in the early recognition and effective management of post-stroke depression. While some only tested the feasibility of the tools in terms of fidelity and acceptability used for assessing different information of the post-stroke patients (Dijk et al., 2018). While it comes to make critical discussion of the secondary research, it needs to be stated that, what are the limitations and strength of research. These findings are highly useful in developing clear knowledge and understanding of researcher about nurse’ roles in management of post stroke depression. In addition to this, the findings are helpful in improving the overall understandings of researchers about risk factors associated with the PSD condition in which the nurses need to determine as well as eliminate these risks to promote proper mental and physical health and wellbeing in PSD patients. Finding of secondary research has improved the knowledge and understanding of researchers about limitations and risk that nurses can face while involving in treatment of a PSD patient and how nurses can coper up with this situation. The limitations that the researcher has faced in conducting this research is time and fund limitation. The researcher is unable to make more search on collecting relevant articles on research topic due to insufficiency of times allotted for this research. In addition to this, researcher cannot include more relevant articles in this research study due to most of the articles are paid articles that cannot be used due to the insufficient fund allocated for the research.
Chapter 5: Conclusion
Like other qualitative studies on post-stroke depression has analyzed, this research too sticks to the point that very few researches have been conducted in this field. Post-stroke depression affecting the lives of many survivors needs more attention from diverse fields so that effective intervention plans can be implemented. All the literatures have identified the role of nurses as vital in the diagnosis as well as the management. But the lack of knowledge and information in the nurses about the management was noted by many studies. So, proper training and guidance should be provided to the nurses for them to function effectively and efficiently for both the diagnosis and the management of post stroke depression. Some of the literature have prioritized the self-assessment training and educational program for nurses in terms of developing their professional standard to take relevant strategies that will assist the entre healthcare team to manage changing needs of patient with PSD. In most of the selected literature in has been mentioned that depression is the common mental is common result of stroke, the actual cause of this mental illness in stroke survivors is still unknown and obscure. many of the selected literatures have concluded that, PSD is associated with different factors such as biological, social, psychological, cultural and socio-economic factors. On discussing nurse’s roles in managing needs of PSD patients, many selected literatures have concluded that, healthcare authority needs to conduct nurse-led intervention to promote better management of care needs of PSD condition. Some psychotherapies, screening tools, counseling processes are recommended by recent literatures in terms of reducing severity of depression in PSD condition. Nurses play important roles in determining the actual psychology, emotional needs and physical needs of patient with PSD, which assist the psychiatrist to set relevant psychotherapies for these patients to heal their overall mental and physical distress. Some of the best screening tools used by the nurses for post-stroke depression were PHQ-2, PHQ-9, Geriatric Depression Scale (GDS) and Montogomery-Asberg Depression Rating Scale (MADRS). No standard screening tool, particularly for the diagnosis of post-stroke depression, has been developed yet. Whereas, the use of mood scales is highly recommended. The most effective strategies adopted by the nurses identified by different literatures for the treatment of post-stroke depression are listening and talking to the patient, consoling the patient, helping them to deal with self-consciousness issues, boosting their confidence and supporting and encouraging them for different therapies like drug therapy, psychotherapy, physical therapy and many more. Some of the literatures reviewed showed that a comprehensive management plan should be implemented for the management of PSD. Nurses, families, doctors, psychiatrists and other health care providers should all join hands for fighting post-stroke depression. Through developing three relevant themes, this research has not only made the comprehensive discussion on nurse roles in management of patient with PSD, but also mentioned the important tools and techniques that can be used in treatment of PSD patients. The finding and discussion of these finding have concluded that, overall roles of nurse in management of PSD patient is not only associated with developing innovative clinical intervention and psychotherapeutic tool, but also associated with regular self-assessment as well as training of nurse to improve the standard of care and treatment process. Here in this research some of the selected literatures have mentioned the limitations and drawbacks that are associated with roles of todays nurse in treatment of PSD patients. Consistent modification of overall treatment process provided by nurse and health professionals to the PSD patients is recommended by many literatures. based on these literatures, regular modification can assist nurse to make proper modification as well as improvisation of care process which will meet the changing critical health needs in PSD patients. Some of the literatures have concluded that, in terms of managing the health needs of PSD patient burse needs to develop innovative communication and interaction process in the workplace which develop the transparent information delivery system in the care homes. Transparent communication and interaction are important for sharing information between nurses and health professional thereby assisting the nurses to take effective strategies and innovative care settings to meet critical needs of PSD patients.
In conclusion, Post-stroke depression is a psychological problem with high prevalence and incidence rate so it is necessary to be dealt with high caution and sensitivity. Implementation of effective strategies by the nurses can be the key to deal with it and reduce the rates.
Reference List:
Atique-Ur-Rehman, H. and Neill, J.C., 2019. Cognitive dysfunction in major depression: From assessment to novel therapies. Pharmacology & therapeutics.
Harrison, M., Ryan, T., Gardiner, C. and Jones, A., 2017. Psychological and emotional needs, assessment, and support post-stroke: a multi-perspective qualitative study. Topics in stroke rehabilitation, 24(2), pp.119-125.
Hussein, A., Idris, I., Abbasher, M., Abbashar, H. and Abbasher, K.M.A., 2019. Post stroke depression. Journal of the Neurological Sciences, 405, p.70.
Karamchandani, R.R., Vahidy, F., Bajgur, S., Vu, K.Y.T., Choi, H.A., Hamilton, R.K., Rahbar, M.H. and Savitz, S.I., 2015. Early depression screening is feasible in hospitalized stroke patients. PloS one, 10(6).
Loft, M.I., Poulsen, I., Martinsen, B., Mathiesen, L.L., Iversen, H.K. and Esbensen, B.A., 2019. Strengthening nursing role and functions in stroke rehabilitation 24/7: A mixed‐methods study assessing the feasibility and acceptability of an educational intervention programme. Nursing open, 6(1), pp.162-174.
Towfighi, A., Ovbiagele, B., El Husseini, N., Hackett, M.L., Jorge, R.E., Kissela, B.M., Mitchell, P.H., Skolarus, L.E., Whooley, M.A. and Williams, L.S., 2017. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 48(2), pp.e30-e43.
Tulek, Z., Poulsen, I., Gillis, K. and Jönsson, A.C., 2018. Nursing care for stroke patients: A survey of current practice in 11 European countries. Journal of clinical nursing, 27(3-4), pp.684-693.
Van Dijk, M.J., Hafsteinsdóttir, T.B., Schuurmans, M.J. and de Man‐van Ginkel, J.M., 2018. Feasibility of a nurse‐led intervention for the early management of depression after stroke in hospital. Journal of advanced nursing, 74(12), pp.2882-2893.
Zhao, F.Y., Yue, Y.Y., Li, L., Lang, S.Y., Wang, M.W., Du, X.D., Deng, Y.L., Wu, A.Q. and Yuan, Y.G., 2018. Clinical practice guidelines for post-stroke depression in China. Brazilian Journal of Psychiatry, 40(3), pp.325-334.
Al-Busaidi, Z.Q. (2008) Qualitative research and its uses in health care. Sultan Qaboos University medical journal, 8 (1), pp.11–9.
Aveyard, H. (2019) Doing a literature review in health and social care. 4th edn. London: Open University Press.
Cooper, C. et al. (2018) "Defining the process to literature searching in systematic reviews: a literature review of guidance and supporting studies", BMC Medical Research Methodology, 18(1). doi: 10.1186/s12874-018-0545-3.
Grewal, A., Kataria, H. & Dhawan, I. (2016) Literature search for research planning and identification of research problem. Indian journal of anaesthesia, 60 (9), pp.635–639
Igwenagu, C. (2016) Fundamentals of Research Methodology and Data Collection. LAP LAMBERT Academic Publishing.
Karamchandani, R. et al. (2015) "Early Depression Screening Is Feasible in Hospitalized Stroke Patients", PLOS ONE, 10(6), p. e0128246. doi: 10.1371/journal.pone.0128246.
Loft, M. et al. (2018) "Strengthening nursing role and functions in stroke rehabilitation 24/7: A mixed-methods study assessing the feasibility and acceptability of an educational intervention programme", Nursing Open, 6(1), pp. 162-174. doi: 10.1002/nop2.202.
Martins, F.S., Cunha, J.A.C. da and Serra, F.A.R. (2018) Secondary Data in Research – Uses and Opportunities. Iberoamerican Journal of Strategic Management, 17 (4), pp.1–4.
Morin, K. (2014) Nursing education: The past, present and future. Journal of Health Specialties, 2 (4), pp.136–140.
Moule, P., Aveyard, H. and Goodman, M. (2017) Nursing research. 3rd edn. London: Sage Publications.
Prada-Ramallal, G., Roque, F., Herdeiro, M.T. & Takkouche, B. (2018) Primary versus secondary source of data in observational studies and heterogeneity in meta-analyses of drug effects: a survey of major medical journals. BMC Medical Research Methodology, 18 (1), pp.1–14.
Teherani, A., Martimianakis, T., Stenfors-Hayes, T., Wadhwa, A. & Varpio, L. (2015) Choosing a Qualitative Research Approach. Journal of graduate medical education, 7 (4), pp.669–70.
Terrell, S.R. (2012) Mixed-methods research methodologies. Qualitative Report, 17 (1), pp.254–265.
Towfighi, A. et al. (2017) "Poststroke Depression: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association", Stroke, 48(2). doi: 10.1161/str.0000000000000113
Mitchell, P. (2016) "Nursing Assessment of Depression in Stroke Survivors", Stroke, 47(1). doi: 10.1161/strokeaha.115.008362.
Van Dijk, M. et al. (2018) "Feasibility of a nurse‐led intervention for the early management of depression after stroke in hospital", Journal of Advanced Nursing, 74(12), pp. 2882-2893. doi: 10.1111/jan.13806.
Williamson, K. & Johanson, G. (2018) Research Methods. 2nd Edition.
Zhao, F. et al. (2018) "Clinical practice guidelines for post-stroke depression in China", Revista Brasileira de Psiquiatria, 40(3), pp. 325-334. doi: 10.1590/1516-4446-2017-2343.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts