Findings on Healthcare Logistics Improvements
Findings
Introduction
The last chapter looked at the results of the study based on the data collected from the case studies. In the methodology section the details of the procedure for collection of data from the responsive individuals of the five nursing homes were taken into consideration. In this chapter we have analysed the findings based on literature review highlights and case studies observations. Three sets of comparisons are presented: 1) a comparison of case characteristics; 2) a comparison of interventions; and 3) a comparison of impact factors. First, the case studies are introduced and case characteristics, which include process descriptions and challenges in healthcare logistics, are compared. Interventions for improving healthcare logistics processes are then reported. Based on the challenges and interventions, impact factors for improving healthcare logistics processes are identified, consolidated and compared across numbers. Suggestions for applying the impact factors as decision criteria for improving healthcare logistics processes are provided and Part II of the final framework is developed. Finally, a chapter summary is provided.
Comparing Case Characteristics
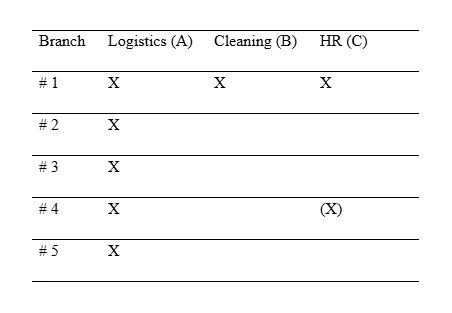
The case study nursing homes are described in Table xx which also provides an overview of the case study. The case study A indicates how many residents each nursing home can occupy, the number of actual residents, the number of rooms that are cleaned per day.

The private nursing home is owned by a non-profit organisation with branches located across the United Kingdom and abroad. For Case B, nursing home 1 was the main case, but limited additional data was collected from another major nursing home. As mentioned within the section of methodology the research investigation was carried with the aid of triangulation process or also mixed methodology. Therefore the findings of the case studies were collected from multiple sources to justify the method adopted. For the case study A the findings were assorted from varied sources of five private nursing homes in the UK, for the case study B the data was assorted from one private nursing home and for the case study of C, findings were collected from the primary nursing home. In this regard this must be mentioned that, Case C, nursing home 1 was the main case, but additional data was collected to a limited extent from nursing home 4 as mentioned above for Case B. The findings were analysed comparatively for all the hospitals with regard to the procedural management of the HR and the logistics section. Leading contextual investigation research involves a few restrictions, for example, speculation issues. Contextual investigations focus on expository instead of measurable speculation. The objective is not worldwide generalisability however to decide under which conditions certain results can be anticipated (Pohjosenperä, 2019). The speculation of contextual analyses happens at a calculated level, not just at the degree of a particular case. The diagnostic speculation of a contextual investigation depends on either the progression of hypothetical ideas, for example through substantiation, alteration or dismissal, or on new ideas rising up out of the contextual investigation (Pohjosenperä, 2019). In this investigation, explanatory speculation depended on both the headway of existing ideas and the recognizable proof of rising ideas. To improve outside legitimacy, various contextual investigations were led. The ID of examples across cases, for example the distinguishing proof of effect factors for the situation examines, improves outside legitimacy (Brax, et al., 2017), and the utilization of a contextual investigation convention improved the outer legitimacy of this examination (Pohjosenperä, 2019).Thus, each contextual analysis sums up discoveries as per the researched procedure and the nation setting.
Table xx Overview of the nursing homes contributing to each case study
A brief description of each case study is provided below. The descriptions include explanations of the process and listings of the people involved. The challenges involved in the processes, the technologies implemented and other improvement initiatives are discussed in separate sections in this chapter.
Case A: The Cleaning Process
The cleaning process in healthcare facilities, as described by Griffin (2018), poses a number of challenges, including how the facilities should be cleaned and the risks staff face in these facilities. Other challenges include training to mitigate physical and health-related risks and the required documentation and supervision (Galligan 2018). Intensive training is required, in addition to documentation such as checklists and written standard operating procedures to validate that the work is completed as specified and this process is maintained throughout the year. Quinn (2019) emphasised that cleaning in healthcare environments poses greater risks due to the nature of the work, including exposure to infectious material and increased risk of fall injuries. According to Martin (2016), although healthcare facilities exist only to provide care to patients, it can come as a surprise to know that logistics cost is typically the second largest expense such facilities incur, exceeded only by the cost of staff. The table provided above for Case A detailed about the five different nursing home branches with respect to the number of residents that they have the capacity to offer space in comparison to the actual number of residents accommodated, and the number of times the rooms are cleaned by the staff members. It was observed that the nursing home branch 1 have the capacity for 35 rooms but the number of residents it provided space was 25 and the staff cleaned the rooms about 7 times each day. Similarly for the branch 20 rooms were there and it provided space to 15 residents and the staff cleaned the rooms about 7 times each day. However, nursing home branch 4 have 7 rooms and provided space to 7 residents and the rooms cleared were 4 times per day and it was even lower for nursing home branch 5 which was cleaned 3 times per day. In this regard, Lapointe (2017) added that the traditional healthcare logistics model is fragmented, hampered by conflicting goals and (in the main) operated under the auspices of nobody in particular and orders are typically placed by different factions within a single facility, and fulfilled by multiple manufacturers, wholesalers and distributors. The top healthcare supply chain management challenges for provider organisations as advised by Lapointe (2017) include provider preference items, a lack of supply chain health IT, and invisible costs. These are the factors that might hamper the interventions undertaken for improving healthcare logistics processes that might result in lower values of impact factors. It can be seen clearly comprehended from the data table of Case A that with there is miscommunication among the staff members of the hierarchy with regard to organisation’s supply chain management process. Moreover, due to the rising cost associated with the elevated level of staff members and moreover this is surely a matter of concern as it is a major part of infection prevention and control (IPC) and belongs to the Healthcare Cleaning Forum 2018 (Peters, 2018). It is also evident from scientific background that a maximum case (50 – 70%) of the hospital acquired infections (HAI) occurs due to the transmission of contamination or pathogenic microorganisms due to the poor hygiene maintenance (Grol, et al., 2013). Moreover about 30 – 50% of the cases are attributed to the transmission by environmental strategies. The study findings also clearly indicated that without the proper cleaning of surfaces in a routine interval manner, there occur a dynamic exchange of pathogenic microbes in between the contaminated surfaces and hands of the staff members or the patients (Pittet, et al., 2006).
The nursing home cleaning process consists of three overall steps, as illustrated in Figure xx:

The first step of the cleaning process is the arrival of a cleaning staff member and cleaning gear at the place to be cleaned. The room is then cleaned by an individual from the cleaning department according to prescribed cleaning standards by following a set of guidelines. It is expected that a certain amount of time is spent on cleaning a room to ensure that cleaning is performed to a satisfactory standard. For quality assurance purposes, a random sample of rooms is checked daily according to a quality check list. The quality of cleaning is important for the nursing home as a step to contain infections and prevent them from spreading throughout the nursing home. However, these procedures are time-consuming and it is difficult to check the quality of a performed cleaning task, so only a sample of rooms is checked (Peters, 2018). The hygiene of the hospital environment is a critical perspective and depends on varied factors such as what is required intervention adopted, the strategy used for the application of the intervention, the degree of contamination present in the environment and the category of the surface and at last another important aspect is the hygiene of the personnel performing the task (Lytsy, 2018). If there is lacking found within any of the above mentioned factors the cleaning process is considered to be suboptimal level. It is because of this reason a multimodal strategy is suggested which considers all of the above factors for the cleaning process of the nursing homes and hospitals (Lytsy, 2018). According to the recommendations suggested by varied researchers on the cleaning aspects of hospitals, the environmental hygiene should be maintained by following the principles of World Health Organization (WHO) model which highlighted about the “Clean Care is Safer Care” that was formulated with respect to hand hygiene in the year, 2005. However, it should be also worth mentioning that few scientific evidences are there that contributed to this field but those are enough to correlate between the cleaning and hygiene of hospitals and the rate of hospital acquired infections (Kilpatrick, et al., 2017).

It is difficult to ascertain whether a room has been cleaned satisfactorily because it may look clean without actually being clean. Taking a biological sample for testing is an even more elaborate and time-consuming task, and so this procedure is conducted less often. The only measures documented for the cleaning process are therefore time stamps for cleaning certain types of rooms and the performed quality checks of a sample of rooms. Over time, adherence to quality is not measured per employee and per unit. Thorough environmental cleaning and disinfection of rooms and communal areas is essential, as advised by Ling and Hui (2019), in order to remove bacterial contamination from environmental and equipment surfaces where residents receive care and thereby prevent the transmission of microorganisms between residents, from residents to healthcare workers and from residents to visitors. The above given graphical figures detailed about the direct association in between the number of infection cases and the failure of hygiene maintenance within hospital environment (Peters, 2018). Few studies have also correlated that patients had fallen sick if the room was pre contaminated with pathogenic hospital acquired microorganisms (Quintana, et al., 2006). They also provided detailed information with regard to the different disinfectants used for cleaning and also upon their efficacy to kill the pathogens. These investigations were basically based on toxicity analysis of the compounds against the pathogens and the specialised strategies to control the outbreaks within healthcare settings. However, with the enhanced level of strategies with regard to cleaning of environment and thorough decontamination strategies which are usually applied to curb down the outbreaks, the impact is very difficult to comprehend (Schoenfelder, et al., 2011). Moreover, in the year, 2018 the network of the European countries formulated an intervention for the promotion of the strategies that should be adopted to provide safety to the patients, and also revised that how the varied hospital network are working to abide by the guidelines (EUNETIPS) (Campione, 2018). The varied products that are available to clean and disinfect the nursing homes and hospital settings are commonly alcohol, chlorinated compounds, glutaraldehyde, formaldehyde, iodophores, hydrogen peroxide, peracetic acid, ortho-phthalaldehyde, quaternary ammonium compounds and phenolics. The concept on the ideal product is considered to be a compound that is effective against any microorganisms, such as the bacteria, viruses, prions, spores but it will have no harmful impact upon the immediate environment (Mitchell, et al., 2018). However no such compounds exist as per the exact definition provided. Apart from the chemicals available for cleaning and their efficacy there is another component on the biological aspect, i.e., the human component which is another important aspect as cleaning is not solely depended on the chemicals used but also upon the personnel who is carrying upon the task. The personnel who are carrying on the task should be very meticulous about it as it is a monotonous job. The figure that was shown for the cleaning purpose highlighted about the overall three processes, i.e., preparation for cleaning, cleaning or disinfecting the rooms as per the standard procedures, and then quality checking. In all the aspects it depends on the person who is carrying on the task as how meticulously the work is being conducted and the products that were used for cleaning. Moreover, the job of cleaning and disinfecting is considered to be a repetitive and mundane task, and with the utilization of unskilled persons for the job the hospital or the nursing homes often put the aspect of patient safety at risk. Another constrains that are faced by the personnel who are appointed for the cleaning and disinfecting job is the time allocation for each time performance of the task and the entire day work load on them that also includes the urgent services required. However these personnel who are responsible for the environmental cleaning of the healthcare setting are on the lowest category of the hierarchy and often they are not provided with the due respect and consideration that they deserve based on the gravity of the work done. The interview based sessions also highlighted that they are considered to be the menial persons of the organization and also uneducated by the other staff of the hospital. However it should be also noted that in varied highly developed countries, the appointed individuals for the cleaning purpose are resourced from other countries and due to this they cannot properly interact with the other staff members properly which even creates more problem. Another most important feature is that there are very few hospitals that have proper infrastructure to properly educate their staffs and provide certificates to them. It is also evident that without proper infrastructure and certification of the training and education, the process is considered to be incomplete for the development and progress of the organization (Schoenfelder, et al., 2011). It has been also noticed with respect to the cleaning staffs that there are high number of turnover rates among those personnel and the language acts as a barrier between them and the other staff members of the organization. There is one recommendations obtained from the study that the individuals who are appointed for the cleaning and disinfectant should be properly educated about the gravity of the work and how it will severely impact the organization progress if carried on with lack of concentration and without taking adequate measures. They should be also provided with the due respect of the work they are performing as they are contributing to the success of the organization (Haque, et al., 2018).

The raised cost related to hospital cleaning process:
It is very much essential to formulate an effective planning for the disinfectant process of the hospital environment. As the introductory investment can offer much more returns afterwards as the promotion of the hand hygiene have resulted about 23 times more success. So as to have comparative figures for emergency clinic ecological cleanliness, we have to initially comprehend what the expense of keeping up a spotless medical clinic condition is, and what its worth is. Albeit numerous medical clinics rush to burn through cash on new programming, specific staff and extravagant gear, they regularly take a gander at keeping up nature cleanliness as a chance to spare in the financial plan (Pittet, et al., 2004). Emergency clinics regularly attempt to cut natural cleanliness support costs however much as could reasonably be expected, both in the items that they use, and in the preparation and proceeded with training of their workforce. The basic move in approach needs to occur in how emergency clinics evaluate this expense and worth. Since the expenses of not cleaning can influence various financial plans inside an emergency clinic, it is hard to precisely represent them. Clinics need to look past genuine uses to deflected consumptions, for example, increment in quiet days due to HAI, just as happenstance costs, for example, emergency clinic staff time or missed careful income because of expanded turnaround time in a surgical theatre. There are likewise increments in costs related with antimicrobial obstruction in HAI, which has an expense assessed at over €85 trillion ($100 trillion) all inclusive by 2050. For instance, one moderately little flare-up with around 40 cases cost a medical clinic over €1 million. Anticipation is in every case preferable and more affordable over a fix, particularly when we are coming up short on anti-microbial. So when settling on a choice about which natural cleanliness support frameworks to purchase, which items to utilize, or the amount to put resources into preparing the cleaning faculty, emergency clinics would do well to take a gander at the expenses of not doing as such, or choosing a less expensive arrangement. So as to set aside cash in the long haul and improve understanding fulfilment, medical clinics need to put resources into quality no matter how you look at it whether in materials, disinfectants, mechanical development, or the preparation, training, and confirmation of their workforce (de Rezende, et al., 2012).
Case B: The Logistics Process in the Primary Nursing Home
According to a survey done by Cardinal Health (2017), an American healthcare services company with branches worldwide including in the United States, the United Kingdom and Europe, while only one-third of the 150 surveyed health care provider leaders described their organisation’s supply chain management process as ‘very effective’, about two-thirds strongly agreed that improving healthcare supply chain management would lower costs, boost revenue and improve care quality. Cardinal Health (2017) also pointed out that many healthcare organisations face some roadblocks in their efforts to make their supply chains more efficient. Some of these challenges include costly provider preference items, a lack of IT implementation for supply chain functions and limited hidden costs transparency. The table of Case B xx detailed about the logistic process that are carried out within the branches of nursing homes. The table on the review of the nursing homes that are contributing to the procedures of the logistics, it was observed all the five branches of the nursing homes have contributed to this process. The findings of all the branches have been assorted for analysis, however for the cleaning and HR management process the data obtained from the nursing home branch 1 and 4 were utilised (Bal, 2015). The position of the environmental hygiene services in a hospital setting is significant from the point of view that how it coordinates its service with the department of IPC service. It was also observed that the nursing assistants are primarily responsible for cleaning one part of the surrounding of the patients whereas the other half is usually maintained by the environmental hygiene individuals. Still there is clear definition of the job functioning among the respective staff members with regard to this role within the hospital setting. Few instances can explain the existing problems such as there are no specifications that one should perform the cleaning process of the table beside the patients. Similarly in a past one survey it was reported that 1/3 rd of the hospital cleaning staffs were not clear about their functioning and their respective responsibility (Strassle, et al., 2012). The supply chain is the process that in what procedures the resources are acquired and in what measures they are supplied to the consumer. This means that the process is mainly based on the ways how the products are transferred from the manufacturer to the patients. The logistic process of the nursing homes is mentioned within the following diagrammatic representation, Figure xx, i.e., the flow of goods from the stock to the storage department and from there it is transferred to the respective departments according to their demands. However it is also clear that the improper management procedures along with the shortage of the necessary staffs makes an hazy situation more complicated and that eventually results in the failure of the critical maintenance. These errors within the whole process lead to transmission of the disorders, starting from a minor mistake to eventually a huge mistake among all the staff members within the healthcare setting. In a healthcare sector several staffs are resourced from outside the nursing homes from varied outside human resourcing companies, therefore it is critically essential for the management to supervise whether the right procedures are being maintained or not in the essential areas by the skilled persons even though the cost of the process in the introductory phase is higher (Mann, et al., 2014).

Dichiara (2017) thus emphasised why healthcare needs a value-based logistics management system and that the holistic flow of relationships between suppliers and customers is about efficiently delivering low-cost care in the form of goods and supplies (such as pairs of gloves) moving from point of purchase to point of use. Vahedian (2017) advised that implementing data analytics and automation tools may make logistics management much easier, as automation allows staff to spend more time delivering high-quality care and less time squirreling away their favourite products just to ensure they are available when required. The logistics flow in the primary nursing home illustrated in the figure xx detailed that when products arrive daily with different barcodes on them, all in different formats, figuring out how to read them becomes an arduous task and often involves the use of different scanners. Kieweit (2018) suggested that the solution may lie in properly assessing supply and demand, understanding what products to order or not order and when according to residents’ needs, resulting in more accurate spending. This new and improved logistics approach will improve materials management and be much more advantageous for residents’ outcomes in the long run. At the point when such a procedure is going all out, physical merchandise and data about pharmaceutical items and administrations travel to some free partners, including producers, insurance agencies, emergency clinics, suppliers, bunch buying associations, and other administrative organizations. Be that as it may, by spilling effectiveness in the territories of the healthcare flexibly chain, clinical associations and private medicinal services suppliers can significantly profit by the general practice. They extend cost-diminishing open doors over their association through this. We feel the motivation to signify this that the medicinal services industry has been working with providers during the time to pick up the edge in consistence that can be conceivable by belittling the rising pattern of significant expenses and wasteful aspects (Bal, 2015). These destructive changes happen due in huge part to declining repayments for administrations. Subsequently, they are looking for chances to lessen costs without reducing the nature of patient consideration, the Supply Chain Quarterly clarifies. Be that as it may, over the most recent few years, things appear to be improved for the advancement. The manner in which human services associations source supplies and speak with makers and specialist co-ops is experiencing an exhaustive change – they stand one that is fundamental to fulfil developing patient needs, address social insurance enactment, bolster a general spotlight on improving patient consideration, and diminish medicinal services costs. As per Gartner's 2016 Healthcare Provider Supply Chain Outlook, we bring to highlight the first worries of the social insurance industry pioneers:
Adjusted targets following vital objectives and incorporated conveyance systems.
Organize normalization.
Lessening pharmaceutical expenses (Min, et al., 2016).
With regards to understanding the difficulties in a steady progression that are influencing the development of the human services industry, so there are scarcely any basic ones:
Expanding government guidelines and prerequisites,
The pharmaceutical patent precipice,
Industry union, fakes
Industry contaminants and venture into developing markets (Min, et al., 2016).
With these difficulties comes the zenith openings and for the medicinal services maker as well as for the coordination supplier. Especially for coordination suppliers, there are plentiful open doors in the medicinal services industry. Back in the time evaluated at €57.9bn, the 2013 pharmaceutical coordination advertise became 11.1% from 2012. Accomplishment of this development depended on the critical factors, for example, the ascent in temperature-delicate pharmaceuticals and venture into developing markets. One may think that it’s difficult to accept, yet it was the developing markets that demonstrated the best year-over-year development with Asia-Pacific (barring China and Japan) driving the way developing 18.5%, Brazil becoming 16.1% and China with 14.3%. Simultaneously, the clinical gadget coordination showcase, evaluated at nearly €20bn, likewise experienced a decent development rate at 14.4% from 2012. Despite the fact that the moderate open doors unleashed are extraordinary; still, coordination suppliers ought to demonstrate their incentive through their insight and reasonable skill. Likewise, they should offer the required types of assistance to laidback social insurance organizations in developing markets to make them sparkle all around. Healthcare expenditures are expanding because of a maturing populace and more refined advances and medicines. Simultaneously, patients anticipate top notch care at a reasonable expense. The medicinal services industry has along these lines experienced expanding weights to lessen the expense of healthcare sector expenditures arrangement while giving great consideration. Co ordinations exercises in clinics give a critical chance to cost control in medicinal services through the usage of best practices (Joshi, 2015).
Interventions that are identified:
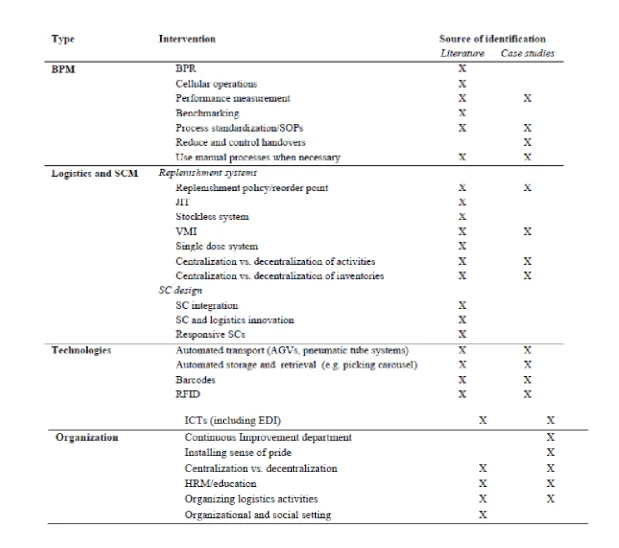
Mediations for improving human services coordination forms were recognized in the writing survey and contextual investigations as detailed in the Results. The distinguished mediations can be separated into four classifications speaking to changes to procedures, coordinations and SCM angles, advances and hierarchical viewpoints. The intercessions can be seen as components of coordination forms in emergency clinics and can add to describing those procedures. Consequently, the procedure mediations depict parts of the procedure structure. Moreover, the researched procedure types complete coordination exercises. At long last, advancements and staff assets play out the coordination exercises. Each sort of intercession is talked about in the accompanying.

Business Process Management interventions:
A few creators contend that a procedure approach is hard to receive in human services settings because of the perplexing condition and request vulnerability (Aronsson et al., 2011; Lillrank et al., 2011). In any case, the writing audit indicated that BPM approaches have been effectively applied in a human services coordination setting, including BPR, cell activities, execution estimation, benchmarking, and process normalization. Furthermore, the contextual investigations included prescribed procedures, for example, diminishing and controlling handovers to guarantee control of the procedure and to lessen the danger of slip-ups. Medical logistics coordination procedures could be benchmarked by operationalizing the distinguished effect factors. Consequently process improvement draws near pertinent in medical services setting may probably apply to medical coordination. One model is the utilization of lean in medicinal services (Souza, 2009), albeit lean in medical procedures will in general spotlight on the apparatuses and procedures of lean as opposed to a framework wide usage (Radnor et al., 2006, 2012).Lean and other administration methods of reasoning receive a quality methodology. Another quality methodology is TQM, which studies have demonstrated is appropriate in a medicinal services setting, for example (Smith and Offodile, 2008; Xiong et al., 2015). An elective quality related methodology material in a social insurance setting is six sigma (Taner et al., 2007), albeit an overview of patient coordination in Dutch emergency clinics shows that six sigma is one of the least actualized improvement draws near (van Lent et al., 2012).

Logistics and Supply Chain Management interventions:
The coordinations mediations distinguished in the writing audit identify with either renewal frameworks or SC structure. Mediations identified with renewal frameworks incorporate recharging strategy, JIT, stockless framework, VMI, and a solitary portion framework. Mediations identified with SC configuration incorporate SC coordination, SC and coordinations development, and responsive SCs. For the contextual investigations, the renewal strategy was spoken to using reorder focuses. Besides, decentralization and centralization of the two exercises and inventories were huge contrasts distinguished between the contextual investigations. Firmly identified with inventories is the idea of decoupling focuses (Rahimnia and Moghadasian, 2010). Towill and Christopher (2005) think about the decoupling focuses for the flow of patients. These decoupling focuses can guarantee that various pipelines of healthcare or medical services conveyance don't meddle with one another, in this manner maintaining a strategic distance from interruptions (Towill and Christopher, 2005). Essentially, decoupling focuses might merit mulling over for social insurance coordinations. Aronsson et al. (2011) found that for persistent streams, it is beyond the realm of imagination to expect to be lean before the decoupling point and coordinated after the decoupling point. They embrace a somewhat extraordinary way to deal with lean and nimble SCs, contending that the medicinal services SC on account of patient streams ought to be separated into sub-forms as indicated by division limits. Qualities of each procedure, for example, fluctuation and volume should then decide if a given sub-procedure ought to be coordinated or lean. Comparable to SC configuration, planning a responsive SC was distinguished as an intercession in writing. Callender and Grasman contend that a responsive SC may be better than a productive cost-centered SC. Be that as it may, a responsive SC doesn't really infer high stock levels. Their examination found that 33% of medical services suppliers experienced incessant crisis orders in view of stock outs (Callender and Grasman, 2010). Responsiveness was not a specific issue for the situation examines. Notwithstanding the coordinations and SCM mediations distinguished in writing, medicinal services coordinations procedures may profit by rehearses found in the assembling business. SC models embraced from assembling may need to adjust to an assistance situation, for example, medical or welfare services. Be that as it may, Aitken et al. contend that both assembling and administration ventures battle to accomplish consistent flexibly chains and that there are a greater number of similitude than dissimilarities among administration and assembling from a SCM point of view (Aitken et al., 2016).
Technology interventions:
The applied advancements distinguished in medicinal services coordinations writing incorporate computerized transport, for example AGVs and pneumatic cylinders, computerized capacity and recovery, standardized identifications, RFID, and ICTs when all is said in done. Comparable advancements were recognized for the situation concentrates notwithstanding clothes washers and gear to stack and empty sleeping pads. Be that as it may, different advancements could apply in a human services coordination setting, for example in enterprises at the edge of computerization, for example, production (van Lent et al., 2012).
Organizational interventions:
The sorts of hierarchical intercessions recognized in writing incorporate arranging coordination exercises, for example figuring out which offices do coordination exercises, HRM, centralization versus decentralization, and authoritative and social setting. As far as sorting out coordination activities, these exercises were completed by coordination offices for the situation study emergency clinics. Besides, the medical clinic wide presentation of a Continuous Improvement division gave a consistent improvement culture and stage for development activities. The centralization versus decentralization angle was additionally recognized for the situation examines; the hierarchical structure of coordination exercises was principally concentrated, despite the fact that inventories and exercises could be incorporated or decentralized. The investigation found that BPR, work re-designing, JIT, and hierarchical rebuilding were the least actualized administrative ways of thinking in the overviewed emergency clinics. The most executed improvement ways of thinking were TQM, constant improvement and benchmarking. Revenue driven emergency clinics announced more accomplishment with executing TQM, BPR and occupation re-building than non-benefit medical clinics, though non-benefit emergency clinics had encountered more accomplishment with hierarchical rebuilding than revenue driven clinics. Both medical clinic types indicated more comparative achievement rates for benchmarking, persistent improvement and JIT. These discoveries show that various kinds of progress ways of thinking are appropriate in a social insurance setting. Of the researched administrative ways of thinking, work re-building was the main strategy not recognized in this examination. Another intriguing finding of the examination is that the accomplishment of the execution relies upon the unique circumstance and possibilities of the medical clinic. So also, the investigations led for this postulation were done for various nation settings and procedure types Smith and Offodile, 2008.
Benefits can be identified for interventions and approaches for improving healthcare logistics processes:
Past scientific evidences gives little direction on the best way to improve human services coordination forms. This examination researches coordination forms in emergency clinics and intends to give hypothetically and experimentally based proof for improving these procedures to both extend the information base of human services coordination and give a choice instrument to medical clinic coordination chiefs to improve their procedures. The writing survey and the outcomes of the investigation distinguished advantages for every intercession. In the writing audit, the accompanying nine kinds of advantages were distinguished: 1) process execution and cost reserve funds, 2) quality, 3) stock administration, 4) stream the executives, 5) tolerant consideration, 6) compliance, 7) staff, 8) acquisition, and 9) data the board and SC coordination. The advantages distinguished for the situation considers were recognized alongside purposes behind actualizing meditations. Therefore, the advantages identify with the effect factors distinguished in this investigation, which thus identify with coordination, advances, forms and hierarchical structure. Out of the 24 recognized effect factors, the recognized advantages identify with everything except two effect factors, to be specific personal time and upkeep and use of advancements. Likewise, the advantages recognized for the situation studies would improve in general execution of coordinations forms as far as productivity and viability. As noted in the Introduction, cost control and great consideration are significant worries inside medicinal services (OECD, 2015; WHO, 2010). Quality is reflected in the advantages recognized both in the writing survey and the advantages distinguished for the situation examines. Besides, the advantages recognized in the Literature Review and the Results identify with costs as far as proficient usage of assets. In addition, all the clinics would give financial defence to any expected interests in intercessions.
Case C: The HR Process
A range of organisational units are involved in the logistics process. The operations department is responsible for the logistics process, including actions such as ordering and replenishing supplies. The cleaning department cleans the rooms and facilities and is responsible for health and safety. The transportation department is responsible for transporting goods such as stock and equipment.

As seen in the HR process implemented in Case C, there is not enough cross-departmental communication. Stark (2019) recommended different ways to improve cross-departmental communication and team work, including holding focus groups, emphasising solutions to the team rather than dwelling on problems, implementing action plans and meeting frequently and Rosenstein (2019) advised that team collaboration is essential and when healthcare proessionals are not communicating effectively, resident and staff safety is at risk for several reasons such as: lack of critical information, unclear orders and misinterpretation of information .
Comparing the Healthcare Logistics Processes
The investigated processes differ in terms of the number of process steps, organisational involvement, level of technology adoption and the nature of the flow.
Centralisation vs. decentralisation
The logistics processes identified in Cases A and C were decentralised and consisted of several different steps, each of which was performed by different departments and required different skill sets. By comparison, the cleaning process in Case B was decentralised, consisted of few process steps and involved only one staff group. The HR process comprised several process steps, although most were carried out by a single staff group. Both cases had decentralised inventories. The logistics process was partly automated and relied heavily on barcodes. By comparison, most of the inventory is stored in storerooms. In addition, automation in the nursing home logistics process provides data which enables performance measurement, data analytics and improvement of processes. The nature of flows. The logistics process consists of a closed-loop flow. For the cleaning flow, staff and equipment are redistributed daily, i.e. in a closed loop, and only cleaning products enter and leave the system. The subjects of the flows also differ in terms of size and variety.
Comparing Challenges in Healthcare Logistics
The challenges identified in the case studies are presented below. First, the challenges identified for the logistics process and cleaning process are presented. These two processes are evaluated together because the cleaning process was to some extent embedded in the logistics cases. Second, the challenges identified in the HR cases are described.
Challenges in Logistics and Cleaning
The challenges of the logistics and cleaning processes are outlined below.
Quality. One challenge experienced is the difference experienced in the quality of cleaning by temporary staff, which is a particular problem during weekends and holiday season. This quality issue is related to the competencies of the employees.
Adherence. Ensuring that employees adhere to SOPs is a serious issue for cleaning tasks. It is imperative that employees spend enough time cleaning each room for quality assurance reasons.
Challenging work conditions. Most of the logistics activities carried out within nursing homes involve demanding physical work and repetitive tasks, and workers are often hard-pressed for time. High rates of absenteeism and employee turnover increase pressure on existing resources.
Challenges in HR Cases
Employee retention. Strenuous and repetitive work is one of the reasons for the high turnover of logistics staff, and it is often a problem for organisations to invest in training their employees only to see them move to another company for a higher salary. However, the managers in this case study perceived this progression as a good thing for employees rather than a loss for the organisation.
Motivation & Employee absenteeism: Logistics and cleaning staff perform repetitive tasks which are physically strenuous. These employees are often viewed by other employee groups as being less important. In addition, the logistics departments often experience high absenteeism rates, due in part to the aforementioned strenuous tasks required in logistics activities. Low levels of motivation may also increase employee absenteeism.
Impact on related processes: One of the goals for the cleaning process is to ensure that the rooms are cleaned sufficiently to help avoid infections from spreading. Thus, the impact on related processes—in this case patient care—is very important to the cleaning process.
Lack of data and performance measurement: Lack of data availability makes it particularly difficult to measure cleaning staff performance, because employees act on their own accord. It is also difficult to measure cleanliness and the time spent on cleaning, making performance measurement challenging for the cleaning process, and the lack of such measurements has led to productivity issues for the logistics process. However, a random sample of rooms are checked according to a quality control check list, and then departments and employees are monitored to ensure that they maintain the necessary standard of quality over time.
Communication and information management: The cleaning department faces a significant communication challenge. First, it is challenging to convince others that a room has actually been cleaned, partly because it is difficult to see whether a room has been cleaned or not and partly because the room may have been cleaned without anyone seeing it. Furthermore, only the cleaning of certain rooms is documented. Second, it is challenging to convince others that the room has been cleaned satisfactorily. Third, the expected level of cleaning is higher than the required level of cleaning. Fourth, personnel often perform more tasks than agreed upon. Creating transparency around what is agreed and what is done is therefore a challenge.
Problematic handover. One employee or organisational unit handing over a task to another increases the risk of mistakes (Hammer and Champy 1993). Correct handovers require that all parties involved are properly trained in how to do so. If different staff groups do not hand over process steps to the next according to the guidelines, such disruptions can lead to more serious problems.
Inefficient processes: Logistics processes are subject to a number of inefficiencies, including unnecessary actions, long waiting time, long transport times, lack of management oversight and inefficient use of resources, balancing priorities which all contribute to low productivity.
Collaborating with and educating other staff groups: The tasks of logistics departments span across the nursing home and employees must learn to collaborate with other staff groups. The handover of a task to a logistics employee affects how that logistics task is handled.
Continuous education: How to cope with the continuous need to educating staff is a problem, particularly as one of the aims of education is to change the culture to one of continuous improvement.
Performance measurement: The difficulty in capturing data makes performance measurement challenging; this in turn makes it impossible to monitor the progress of process improvement initiatives. Traceability in the process would enable better and more frequent performance measurement.
Maintenance. Maintaining centralised technologies is challenging and time-consuming; these issues are exacerbated when the technologies in question are decentralised. Table xx links the identified challenges to the derived impact factors, demonstrating the connections between data and codes.
Summary of Challenges in Healthcare Logistics
The challenges listed below were identified in the investigated case studies and recurred throughout all the cases:
Performance measurement;
Capturing data;
Employee retention;
Employee absenteeism;
Physical constraints;
Locating people and items;
Systems integration; and
Problematic handovers.
These are example of challenges observed, what is perceived as a challenge for one nursing home does not necessarily pose a challenge for another because of the interventions which have been implemented. In the following section, the interventions identified for the case study processes are presented and best practices identified.
Comparing Interventions in Healthcare Logistics
The interventions identified in each of the case studies are presented below, together with reasons for their implementation and their observed benefits. The interventions are divided into the categories BPM, logistics and SCM, technological interventions and organisational interventions, according to the literature review. Each of the interventions is related to the identified impact factors, i.e. data is linked to the codes used for analysing the qualitative data. The identified impact factors served as decision criteria in the framework developed in this study and best practices were identified based on the interventions.
Business process management: The BPM interventions identified for the investigated case studies are presented in the following table. BPM interventions include any implemented changes relating to BPM, including changes to process steps and applied performance management.
The logistics and cleaning BPM interventions are presented below. Table 4xx provides an overview of the interventions and the related impact factors identified from the qualitative data coding.
Logistics and SCM Interventions
The logistics and SCM interventions identified for each of the case studies are presented below. They were treated in conjunction with one another, while the HR cases were treated separately. The logistics and SCM interventions for the logistics and cleaning processes are listed in Table XX along with the reasons they were implemented and their related impact factors. As shown in Table XX, the SCM interventions mainly related to the centralisation and decentralisation of activities and inventories. Table XX. Logistics/SCM interventions and related impact factors for logistics and cleaning interventions to be added xx.
Technological Interventions
In this section, the technological interventions identified for each case study are reported. The technologies identified for logistics and cleaning were treated together and the technologies identified for the HR process were addressed separately. The technological interventions and related impact factors for logistics intervention, reasons for implementation and benefits associated with the derived impact factors are explained below:
Mobile phones. Staff were equipped with mobile phones to prioritise tasks, assign or accept jobs and to monitor their progress. The associated impacts of this factor are information management and traceability.
Barcodes. The use of barcodes made it easier to trace the movement of beds and to implement data capturing, planning and continuous improvement. The associated impacts of this factor are information management and traceability.
RFID. The use of RFID also made it easier to trace the movement of beds and to implement data capturing and planning. Using RFID to capture data is more automated than for barcodes. The captured data related to beds, which enabled planning and the study and improvement of the bed flow. The associated impacts were information management, traceability and the degree of automation.
Some efforts to implement certain technologies failed. For instance, in one nursing home the employees refused to use a piece of equipment because it required a prolonged processing time. In another nursing home, the same equipment failed because it could get wet. RFID was tested in the nursing homes but it was not used in the facilities’ day-to-day operations. Similarly, barcodes were only used to a limited extent and mainly for maintenance purposes. In some nursing homes, further investments in software were necessary to fully utilise barcodes. In the logistics process, few technologies had been implemented and were mainly intended to make physically hard work easier for staff. The nursing home case had mainly implemented technologies enabling transportation and information systems for bed management and performance measurement purposes. The difference in technological interventions partly related to differences in process design, which involved central cleaning to allow for automation of the cleaning process. Another aspect which could explain the differences is that some nursing homes seems more concerned with performance measurement than others.

Organisational Interventions
The organisational interventions identified for the logistics and cleaning cases are presented below, followed by the identified organisational interventions for the HR cases. The organisational interventions for logistics and cleaning mainly related to centralisation of the organisation and competence enhancement. The logistics staff were often not able to see their individual contribution to the overall goals of the nursing homes and did was not necessarily view their jobs as a step toward a future career. The managers of one nursing home had made a particular effort to improve their employees’ sense of worth and to help them realise the contribution each of them made to the facility. Out of all the interventions identified in previous sections, the best practices are discussed in the following section.
Best Practices
The best practices identified in the case studies for each of the four types of interventions are discussed in this section. The purpose of identifying best practices is to elucidate the best opportunities for managers to improve their processes and to provide a number of alternatives for improving healthcare logistics processes, which managers can then choose to implement or not. Whether to implement an intervention depends on the needs and preferences of the nursing home and possible contingent factors, i.e. the circumstances under which an intervention is preferable. It may not be feasible to implement all the identified best practices, so managers may have to narrow down the number of interventions to be implemented. A framework is developed in this thesis to guide decision makers in improving their processes so that they can choose the most suitable interventions suitable for a particular nursing home. The best practices were selected based on the benefits experienced in the nursing homes and the opinions of the interviewees. Other best practices may therefore exist beyond those identified in the case studies, e.g. those discussed in the literature or even some which may have not yet been reported. Furthermore, some best practices may only apply in certain cases, while other practices may apply under several different circumstances. The best practices are discussed according to each of the four types of interventions, i.e. BPM best practices, logistics and SCM best practices, technological best practices and organisational best practices.
BPM Best Practices
The following BPM best practices were identified in the case studies: Performance measurement, SOPs, reducing and controlling handovers, continuous improvement and implementing manual processes when necessary.
Performance measurement: Performance was measured for all case studies. It was found that these processes could benefit from more data capturing to enable better performance measurement and to monitor performance progress.
SOPs: Standard operating procedures were identified for all cases, although in some cases they were followed more stringently than others.
Reduce and control handovers: Apart from the cleaning case, the investigated processes involved several handovers between staff groups, which increased the risk of mistakes. Handing over responsibility for a task also means that accountability is shifted to another employee, so it is important to document who is responsible for which actions at what point in time.
Continuous improvement: Continuous improvement permeated the culture and organisation of the entire nursing home. This approach ensures that process performance is continually improved and that processes are designed to create value for the residents.
Logistics and SCM interventions: The following logistics and SCM best practices were identified in the cases:
Reorder points;
Centralisation vs. decentralisation of activities; and
Centralisation vs. decentralisation of inventory.
Reorder point. A reorder point was set for Such a practice is mainly relevant for tangible items and for processes which are not closed-loop.
(De-)centralisation of activities. The lead time for delivering a clean room for a new resident may be shorter for one nursing home than another, but time to transport the bed to the central cleaning unit is also required. Conversely, a room can only be released to a new resident after the room and bed has been cleaned, possibly leaving no time to transport the bed. In terms of quality, some would argue that the cleanliness of beds improves quality because they can be cleaned using washing machines. Thus, the setup depends on the priorities of the nursing home in terms of these trade-offs.
(De-)centralisation of inventory: This difference can be attributed to differences in process design in terms of centralised and decentralised cleaning activities. For the cleaning process, cleaning gear and products are managed centrally rather than stored locally in departments. In addition, nursing homes hold central stock to supply the decentralised inventories. One reason for this difference could be the difference in the size of a facility, particularly in terms of beds and space. Such a setup would either require the delivery of a massive amount of resources within a limited time span or coordinated deliveries throughout the day.
Technological best practices: The following technological best practices were identified in the cases: Electronic data interchange (EDI), barcodes, RFID and picking carousels. EDI enables nursing homes to order products and complete transactions through a secure line between the nursing home and the supplier. Barcode technology enables managers to track and trace items, although not in real time, and can capture data to enable performance measurement. With regard to RFID, depending on the technical specifications of the RFID solution implemented and the placement of scanners, this technology can enable real-time tracking and tracing of items and personnel and allow for the continuous monitoring of processes. Data capturing through RFID technology also enables performance measurement. RFID was only used in the day-to-day operations of the nursing home and only to a limited extent; greater use of RFIDs, e.g. for inventory management, could provide significant benefits, particularly to enhance stock accuracy and to automate the stock counting process. Finally, the use of a semi-automated picking carousel is flexible and requires less space than a fully automated solution. Nursing homes often have little space to spare, and a semi-automated solution might be preferable in such a setting. However, a picking carousel is only useful for processes involving tangible items.
Education. For all the case studies, training was part of enhancing employees’ competencies. The cases showed that training should not only include logistics staff but also other staff groups such as clinical staff who engage with logistics processes in nursing homes. The case results also show that staff competencies influence the quality of their work.
Consolidating and Categorising the Identified Impact Factors
The impact factors identified in the previous sections of this chapter are categorised below. Interrelations between impact factors are suggested based on the case studies.
The identified impact factors are summarised in Table xx. The impact factors reflect the codes identified in the process of coding the qualitative data. The codes have been categorised according to the four constructs of logistics, technology, procedure and structure, which were identified in the literature review.
Table xx. Identified and categorised impact factors (logistics, technology, procedure and structure)
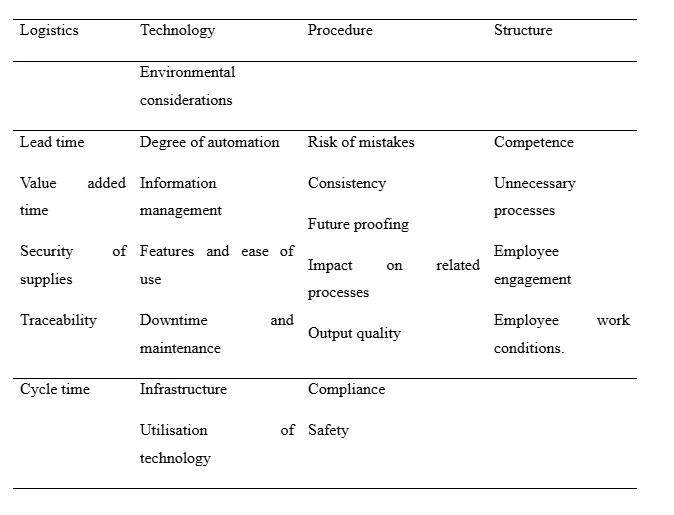
Table xx Description of impact factors across all cases



In addition to being categorised according to the four constructs mentioned above, the impact factors can be divided into efficiency and effectiveness to reflect performance. As previously mentioned, efficiency is input-oriented and requires the economic use of resources, i.e. ‘doing things the right way’. Effectiveness is output-oriented and addresses the extent to which goals have been achieved, i.e. ‘doing the right thing’ (Neely et al., 2005; Mentzer and Konrad 1991; Gleason and Barnum 1982). Table xx shows how each impact factor relates to efficiency and effectiveness, respectively.
Table xx. Categorising the impact factors in terms of efficiency and effectiveness

Arguments for the categorisation of each impact factor in terms of efficiency and effectiveness are provided below, starting with the impact factors relating to efficiency. Lead time, value-added time and cycle time are categorised as components of efficiency. A reduction in any of these measures whilst using the same resources would lead to a better use of resources within a shorter amount of time. However, lead time and value-added time could also be viewed as components of effectiveness in terms of quality and creating value for the patient. Degree of automation is categorised as efficiency because automation can lead to faster production on a larger scale. Downtime and maintenance disrupts production and leads to poor utilisation of technologies. However, regular maintenance is necessary to prolong the life of a technology. Features and ease of use means that a technology is easier to use for employees and provides features which may increase efficiency, i.e. automation. Utilisation of technologies reflects a higher utilisation of a given resource, thereby increasing efficiency. Infrastructure, which in this case can refer to both IT infrastructure and physical infrastructure, relates to ‘doing things the right way’, i.e. efficiency. The risk of mistakes is related to quality to an extent but is categorised as an efficiency measure, as mistakes require the same work to be done again and hence more resources are necessary to perform a single given task. Consistency relates to ‘doing things the right way’ and is thus a measure of efficiency, although it is also related to quality. Future proofing reflects ‘doing things right’ in the long run, meaning that the question of whether a solution will be sustainable for many years to come must be addressed. Competence shifts (handovers) take time and may cause mistakes which require work to be done again, thereby decreasing efficiency. Competence match refers to the required skills to perform a task; lack of competencies may increase the time needed for an employee to perform a task and could lead to mistakes which decrease efficiency. Unnecessary processes are those processes which could be eliminated to reduce the resources needed to perform a task. The impact factors relating to effectiveness are discussed below. Security of supply means that customers or patients will be able to receive any service or item they need (i.e. the output). Traceability does not relate to the economic use of resources but rather the goal of controlling the process and ensuring accountability in a process. Information management may enable the efficient use of resources through the analysis of captured data, but as such it enables achieving a goal. Environmental considerations, some would argue, are consistent with the economic use of resources. However, in this case, additional aspects such as chemicals and effects on the environment must be considered. Output quality refers to producing a better output, for instance in terms of customer needs. Compliance could be viewed as ‘doing things right’, although in this case it does not necessarily mean the economical use of resources, which would make it a component of effectiveness. Safety and experience are part of the overall goals of a nursing home and therefore reflect effectiveness. Employee work conditions do not relate to the economical use of resources; on the contrary, it may be necessary to use more resources to provide better conditions for employees, making this factor a component of effectiveness. Impact on related processes relates to the overall goals of an organisation rather than the efficiency of a single unit. Employee engagement relates to ensuring that employees are satisfied with their work. Some of the impact factors discussed above could relate to both efficiency and effectiveness. The arguments laid out reflect how each impact factor was understood for this study. Although there are other more popular views, the impact factors can nonetheless be related to either efficiency or effectiveness and as such reflect aspects of performance. Thus, the impact factors can be used for performance measurement and benchmarking purposes.
Suggested Relationships between Impact Factors
Each of the identified impact factors relates to the constructs introduced above: logistics (L), technology (T), procedure (P) and Structure (S). Relations between the impact factors were suggested based on the case studies and are presented in Table xx. The proposed relations need further validation, but additional evidence was found in the remaining case studies.
Table xx. Suggested relations between impact factors



The nature of the identified effects between impact factors, i.e. whether the effect of the impact factor is positive (+) or negative (-) is indicated in the far right column of Table xx. The identified effects can be consolidated into a simplified model as depicted in Figure xx

The effects explicated in Table xx and illustrated in Figure xx suggest that logistics and procedure-related factors were influenced the most by other factors (13 and 11 effects, respectively), whereas those related to structure and technology influenced other impact factors the most (13 effects each). These effects need further validation, but they do suggest that in terms of decision-making, the effects between the four constructs occur and should be taken into consideration. This aspect of decision making is discussed in greater detail in the Results. The identified effects indicate that organisational and technological interventions will affect other aspects of a healthcare logistics system the most.
Comparing Impact Factors across Cases
Fifteen impact factors were identified and ranked as decision criteria according to the importance of improving healthcare logistics processes. Five respondents from the logistics case, five respondents from the cleaning case and five respondents from the HR case assigned values on a 0–10 scale. Table xx shows the average (µ) and standard deviation (σ) for each case and across all respondents. The table is sorted according to the average of all respondents, i.e. the far right column. Horizontal lines indicate the top five and bottom five factors. For the most part, the standard deviation increased as the average decreased, indicating that there is more consensus regarding high-ranking factors than low-ranking factors.

The top five impact factors across all respondents are output quality, consistency, employee engagement, risk of mistakes and security of supply. Three of the top five factors (output quality, consistency and risk of mistakes) thus relate to quality. The bottom five impact factors across all respondents were identified as competence shifts, future proofing, competence match, degree of automation, and environmental considerations. Competence shifts and competence match in particular seem to be under-evaluated: These factors significantly impact quality and therefore should receive more attention.
Comparison of Logistics Cases
The logistics cases are compared in Table xx. The average (µ) and standard deviation (σ) for each case has been calculated. To rank the impact factors across both case studies, equal weights were assigned to the results of each case study to calculate an overall average.
Table xx. Ranking of impact factors for logistics cases

Three impact factors reoccurred for both logistics cases: Output quality, employee engagement, and consistency. In addition, employee work conditions and security of supply occurred for the consolidated ranking, where both cases were assigned equal weights. The impact factors reoccurring as least important for logistics cases included degree of automation and competence match. However, the case studies showed that competence match significantly impacted the output quality of a process, suggesting that more focus on this factor is needed. As previously noted, degree of automation is not necessarily desirable, which is reflected in the ranking.
Comparison of Logistics and HR Cases
Table XX compares the ranking of impact factors across the logistics and HR cases. The respondents for the HR cases agreed that information management, security of supply, employee engagement and risk of mistakes are important in improving logistics processes. Similarly, the top five impact factors for the logistics cases included employee engagement and security of supply. Employee engagement and security of supply are thus of high importance for both logistics and HR cases.
Table XX. Comparison of logistics and HR case ranking

There seems to be agreement on the lowest-ranking factors for the logistics and HR cases: Competence match, future proofing, degree of automation and environmental considerations ranked in the bottom five impact factors for both HR and logistics cases.
Summary of Impact Factor Comparisons
Across all respondents, the following impact factors were ranked as the top five impact factors: output quality, consistency, employee engagement, risk of mistakes and security of supply. Similarly, risk of mistakes, output quality, and employee engagement were perceived as the most important decision criteria. The respondents agreed that information management and traceability were among the most important decision criteria, thus differing from the overall ranking of impact factors. The following three impact factors also ranked high: experience and safety, compliance and consistency. Comparing the cases, risk of mistakes, output quality, and employee engagement ranked high, which is consistent with the overall ranking. For the logistics cases, output quality, employee engagement, and consistency rank high as decision criteria. These criteria are consistent with the overall ranking of decision criteria. In addition, employee work conditions and security of supply were relevant to the consolidated ranking, where both cases were assigned equal weights. Security of supply was also consistent with the overall ranking of impact factors as decision criteria. For the HR cases, information management, security of supply, employee engagement and risk of mistakes ranked high as decision criteria. Apart from information management, these decision criteria were consistent with the overall ranking of decision criteria across all respondents. Comparing the logistics and HR cases, employee engagement and security of supply reoccurred for both process types. There seemed to be some agreement on the most important decision criteria within the case studies and process-specific differences. Overall, the lowest ranking impact factors as decision criteria were competence shift, future proofing, competence match, degree of automation and environmental considerations. With the exception of environmental considerations, all identified impact factors were validated as decision criteria for healthcare logistics processes. The degree of automation ranked low for most cases and traceability and future proofing did not seem to be significant. Applying all identified impact factors as decision criteria for improving healthcare logistics processes may be an elaborate task if all decision criteria are to be considered. Thus, identifying the most important decision criteria for particular circumstances can help managers identify focus areas for improvement. A smaller number of decision criteria may be useful in focusing the assessment of possible alternative interventions. Finally, the prioritisation of impact factors can help decision-makers understand the drivers of change in healthcare logistics.
Applying the Impact Factors in Decision-Making
How to apply the various impact factors in the decision-making process of improving healthcare logistics processes is suggested below. The impact factors can be applied to either qualitative or quantitative methods, or a combination of the two in a mixed-methods approach; the suggestions offered below relate to specifically qualitative or quantitative applications. These applications can be applied separately or in parallel for a more nuanced analysis. Meredith and Suresh (2016) suggested three types of justification methods: strategic, economic and analytic. Strategic methods are included here as a qualitative method or descriptive approach. Economic methods are not included, but the suggested analyses are proposed as complementary to an economic analysis. Finally, analytic methods are included as quantitative methods. Another included quantitative approach is the application of impact factors for benchmarking purposes and, by association, performance measurement.
The Qualitative Application of Impact Factors for Assessment
A qualitative application of the impact factors in a decision-making process should include a description of each of the impact factors for different interventions. Comparing the descriptions of impact factors for different interventions to an organisation’s strategy could help align the strategy by selecting a solution which matches the overall strategy and goals of the organisation.
Quantitative Applications of Impact Factors for Assessment
This section explains how impact factors can be used to assess alternative solutions for a healthcare logistics process by applying the ANP method to the identified impact factors. The application of ANP for assessing alternative solutions is exemplified by alternative technologies to be implemented in a distribution process. The ANP method considers the interdependencies between impact factors. A more simplified method is the application of the AHP method or a simple weighted factor model, although this method does not consider the internal dependencies of impact factors. In either case, it would be worth considering how interventions may affect different aspects of the logistical system. The impact factors may not only be used to assess technologies but to assess the entire process design, as technologies are part of the process design. In broader terms, the impact factors may be used to assess BPM interventions, logistics and SCM interventions, technological interventions and organisational interventions.
Operationalisation of the Impact Factors for Benchmarking
The identified impact factors can be operationalised as metrics for benchmarking purposes, using the following categories: quality, security of supply and employee engagement. The quality-related measures include risk of mistakes, consistency and output quality. Variability could serve as a measure of the risk of mistakes, while consistency could represent the allowed variability and output quality could refer to the service level provided, e.g. lead time for transports and service level agreements in general. The security of supply could be measured as the rate of orders fulfilled by suppliers. Finally, employee engagement could be measured as the employee turnover rate and employee absenteeism, e.g. average number of sick days per employee or absence rate. The suggested performance metrics could be used not only for benchmarking purposes but also for pure performance measurement purposes, and the identified impact factors could reflect the efficiency and effectiveness aspects of performance.
The Framework for Improving Healthcare Logistics (Part II)
Part I of the framework developed in this thesis was presented in the Literature Review. In this section, Part II of the framework is developed. In the next chapter, the complete framework is consolidated and presented. Part II of the final framework is based on the results presented up until this point. Figure XX illustrates Part II of the framework, which consists of three steps. First, a manager must decide which process to improve. Second, the decision criteria are applied to the subject being investigated (the process to be improved). As previously described, both qualitative and quantitative approaches can be applied to the impact factors for assessing alternative solutions or improvement approaches. These solutions or improvement approaches can be identified based on Part I of the framework and the interventions identified in the case studies. Complementary economic analyses should be conducted to support the decision process and contingent factors should be considered in narrowing down the number of suitable alternatives. Third, based on the quantitative and/or qualitative analyses, managers should be able to select interventions or approaches for improvement.
Applying all the identified impact factors as decision criteria in the framework may not be feasible in terms of available time and resources, so managers may therefore choose to focus on what they deem to be the most important impact factors. The process chosen for improvement may not be the logistics or distribution process, so managers should look for similarities to these processes in terms of challenges and other process characteristics, e.g. product type, closed- or open-loop processes or country setting. The prioritisation of impact factors may differ for a particular nursing home depending on its type, environment of operation and management or operational strategy. A few contingent factors were identified in the case studies. First, the use of reorder points mainly applies to tangible items and flows which are not closed-loop. Second, the choice to centralise or decentralise activities may lead to a trade-off between increased lead time and increased transport time, as for the logistics cases. Third, the choice between centralised and decentralised inventory may depend on the choice of centralisation or decentralisation of activities. Fourth, applying barcodes or similar technologies may depend on the need and legal requirements to control the process. Fifth, the availability of financial resources is likely to determine whether technologies are implemented.
Chapter Summary
This section replied and talked about the exploration questions researched in this study. This part finishes up on the discoveries of this investigation and offers recommendations for future exploration. The section is organized as follows. To start with, the exploration questions are replied in the finishing up comments. A record of the commitments to explore is then given, trailed by an appraisal of the useful ramifications of the investigation. At long last, a section synopsis is given. The increasing expenses of healthcare or medical services arrangement and the expanding interest for excellent consideration at a sensible expense give the underlying inspiration of this investigation. Co ordinations forms offer noteworthy potential for cost decreases in emergency clinics and are the focal point of this exploration. Also in this chapter, the challenges were identified for each of the case studies, interventions pertaining to BPM, logistics and SCM, technologies and organisational structure were reported and best practices identified. Based on the case study challenges and interventions, factors impacting the decision to improve healthcare logistics processes were identified through coding of the qualitative data. The identified impact factors were then ranked according to importance and compared across cases. Applications of impact factors in a decision process were proposed and Part II of the framework to improve healthcare logistics processes was developed. The commonsense ramifications of this investigation are consequently talked about in the accompanying. Above all else, this investigation gives a system to supervisors to settle on an educated choice to improve human services coordination forms given the setting of an emergency clinic. A rundown of the primary difficulties in medical services logistics forms are given, which can assist chiefs with distinguishing provokes inalienable to their procedures and help centre consideration around any improvement endeavours. To address difficulties and help improve medical services coordination forms when all is said in done, an index of intercessions is given. In light of this inventory of intercessions, chiefs can distinguish the most appropriate improvement mediations given the conditions of the clinic. The conditions under which to actualize changes, for example the relevant factors or impact factors are given to control the choice. Along these lines, the recognized unforeseen variables assist chiefs with narrowing down the quantity of mediations which are pertinent to the circumstance of the supervisor. The discoveries of this examination give bits of knowledge about the components affecting the plan of medical logistics coordination procedures or, put in an unexpected way, the choice of intercessions to be actualized in a human services coordination process. The positioning of the recognized effect factors as choice rules empowers setting explicit dynamic dependent on the created structure. In light of the positioning of effect factors as choice standards, supervisors can organize the rundown of mediations, which has just been limited dependent on the unforeseen elements. Positioning of effect factors as choice measures may contrast across emergency clinics, yet the discoveries of this investigation propose that examples exist for particular sorts of procedures. The prioritization of effect factors gave in this proposal can enable supervisors to figure out where to centre their improvement endeavours. The recognized effect variables can assist supervisors with contemplating and decide regardless of whether their own needs may vary from those distinguished in this examination. Needs might be explicit to a specific procedure or a medical clinic, which the structure permits to be considered. Besides, the recommended interrelations between sway components can assist chiefs with understanding the ramifications of intercessions and view human services forms comprehensively as a major aspect of a framework. The positioning of effect factors gives another use of effect factors, in particular benchmarking. The positioned sway factors empower the system to benchmarking and estimating the presentation of healthcare logistics coordination forms.
Developing the Final Framework
In this chapter, the final framework is developed by merging and consolidating Parts I and Part II, presented in previous chapters. A guide for how to apply the framework in practice is also provided, and the chapter concludes with a summary of its contents.
Consolidating the Framework
Interventions for improving healthcare logistics processes were identified in the literature review and results of this study. The interventions of the literature review and the best practices of the case studies are consolidated into the list provided in Table 5.1.
Table 5.1. Identified interventions in literature and case studies

The interventions identified in the case studies are more detailed than the intervention identified in the literature review. To avoid the summary of interventions for improving healthcare logistics processes becoming too detailed, only best practices have been included from the case studies. Furthermore, a number of contingent factors were identified for the interventions and can be found in Tables 2.7 and 2.8. The final framework consists of six steps, as illustrated in Figure 5.1. The dotted lines indicate optional links between framework elements and will be explained below. In the first step of the framework, decision-makers must decide which process to improve. The dotted arrow between the decision criteria/impact factors and the healthcare logistics process in Step One indicates that impact factors may be used to decide which process to improve, such as by identifying major challenges or using weighted impact factors as decision criteria to identify and prioritise areas for improvement. However, other reasoning may be applied at the discretion of the decision-maker to select a process for improvement, which is also indicated by the dotted arrow leading from the ‘additional analyses’ box. The arrow between contingent factors and the healthcare logistics process indicates that healthcare logistics processes are embedded in a given context. In Step Two of the framework, decision-makers can identify benefits they wish to achieve or challenges they wish to address. The benefits which can be achieved through different interventions, as identified in literature, are listed in Table 2.9 in the Literature Review. Similarly, the challenges identified in healthcare logistics literature are provided in Table 2.5 in the Literature Review. Step Three of the framework matches benefits with interventions. If the point of departure is the challenges in a process, challenges are first matched with the benefits which can alleviate those challenges. Subsequently, the interventions which can produce those benefits are identified.
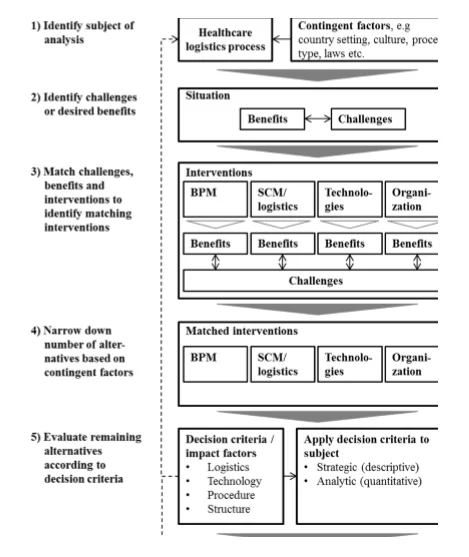
Step four of the framework narrows down the number of interventions from those relevant to achieving certain benefits to those which are relevant under the given circumstances. The contingent factors may relate to process type and country setting, but they should also refer to the entire list of contingent factors listed in Tables 2.7 and 2.8 in the Literature Review. Some interventions which can help provide certain benefits to alleviate a given challenge may not be relevant to a particular problem or situation, so the relevance of an intervention must be taken into consideration. For example, an AGV may not be relevant for the distribution of a service but only for the distribution of tangible items. The application of common sense is therefore an underlying assumption of the framework. In Step Five, the remaining alternative interventions are assessed based on the decision criteria identified in this study. The 24 impact factors, which can be used as decision criteria, can be applied to the healthcare logistics process using either a quantitative or qualitative approach or both. In a quantitative approach, methods such as AHP, ANP or a weighted factor method could be applied. The quantitative assessment can be based on the decision-makers’ own prioritisation of impact factors or on the prioritisations presented in this study. For a qualitative approach, each impact factor could be described and compared for each remaining alternative intervention. Additional analyses, such as economic justifications, may be necessary. In Step Five of the framework, all or only the most important impact factors may be considered. The prioritisation of impact factors presented in the Results can help determine the most important impact factors, such as for a specific type of process and national context. However, other impact factors may be more important to a particular nursing home depending on its specific context. Decision-makers therefore need to decide which impact factors they wish to consider. In the sixth and final step, one or more interventions are chosen for implementation based on the previous steps of the framework.
Chapter Summary
This section replied and talked about the exploration questions researched in this study. This part finishes up on the discoveries of this investigation and offers recommendations for future exploration. The section is organized as follows. To start with, the exploration questions are replied in the finishing up comments. A record of the commitments to explore is then given, trailed by an appraisal of the useful ramifications of the investigation. At long last, a section synopsis is given. The increasing expenses of healthcare or medical services arrangement and the expanding interest for excellent consideration at a sensible expense give the underlying inspiration of this investigation. Co ordinations forms offer noteworthy potential for cost decreases in emergency clinics and are the focal point of this exploration. Also in this chapter, the two parts of the framework developed in previous chapters were merged and consolidated into one final framework. The final framework consists of six steps to improve healthcare logistics processes. The identified interventions, contingent factors and impact factors are inherent to the framework. The common sense ramifications of this investigation are consequently talked about in the accompanying. Above all else, this investigation gives a system to supervisors to settle on an educated choice to improve human services coordination forms given the setting of an emergency clinic. A rundown of the primary difficulties in medical services logistics forms are given, which can assist chiefs with distinguishing provokes inalienable to their procedures and help centre consideration around any improvement endeavours. To address difficulties and help improve medical services coordination forms when all is said in done, an index of intercessions is given. In light of this inventory of intercessions, chiefs can distinguish the most appropriate improvement mediations given the conditions of the clinic. The conditions under which to actualize changes, for example the relevant factors or impact factors are given to control the choice. Along these lines, the recognized unforeseen variables assist chiefs with narrowing down the quantity of mediations which are pertinent to the circumstance of the supervisor. The discoveries of this examination give bits of knowledge about the components affecting the plan of medical logistics coordination procedures or, put in an unexpected way, the choice of intercessions to be actualized in a human services coordination process. The positioning of the recognized effect factors as choice rules empowers setting explicit dynamic dependent on the created structure. In light of the positioning of effect factors as choice standards, supervisors can organize the rundown of mediations, which has just been limited dependent on the unforeseen elements. Positioning of effect factors as choice measures may contrast across emergency clinics, yet the discoveries of this investigation propose that examples exist for particular sorts of procedures. The prioritization of effect factors gave in this proposal can enable supervisors to figure out where to centre their improvement endeavours. The recognized effect variables can assist supervisors with contemplating and decide regardless of whether their own needs may vary from those distinguished in this examination. Needs might be explicit to a specific procedure or a medical clinic, which the structure permits to be considered. Besides, the recommended interrelations between sway components can assist chiefs with understanding the ramifications of intercessions and view human services forms comprehensively as a major aspect of a framework. The positioning of effect factors gives another use of effect factors, in particular benchmarking. The positioned sway factors empower the system to benchmarking and estimating the presentation of healthcare logistics coordination forms.
Discussion and Limitations
In this chapter, each of the research questions is answered and discussed in relation to the extant literature. The meta-RQ is addressed in the answers to the composite RQs, which in turn are answered through the underlying SQs. The limitations of the study are also presented, followed by a summary of the chapter.
Process Characterisation
The first research question (RQ1) is discussed in this section and is formulated as follows: ‘How can healthcare logistics processes be characterised in terms of challenges and composite design elements?’ The research question consists of four sub-questions, each of which will be discussed to answer RQ1.
Challenges
What are the challenges specific to healthcare logistics processes? The case studies and literature review revealed a number of challenges inherent to healthcare logistics. Table xx in the Literature Review lists a set of challenges specific to healthcare logistics processes; some of these are also specific to certain process types. Thus, for nursing home products, challenges include product availability, perishability and product waste, special handling of items and process interruptions. The literature review also provides a list of challenges applicable to healthcare logistics processes in general, the most significant of which include systems integration, ensuring the right skills, overstocking, balancing quality and costs, inventory shrinkage, lack of SC integration, SC complexity, unpredictability, delays, process immaturity, inefficient processes, political agendas and high SC costs. Challenges similar to those identified in the Literature Review were identified in the case studies. However, unpredictability, political agenda and high SC costs were not mentioned as particular challenges in the case studies. Although high SC costs were not perceived as a particular issue, SC costs were indirectly considered an issue particularly for nursing homes due to budgetary limitations. It is worth mentioning that unpredictability and variability in healthcare SC are often the result of both natural and artificial variability in the SC. Unscheduled demand in healthcare is subject to natural variation, whereas scheduled demand may be subject to artificial variation caused by poor nursing home practices. Studies show that unscheduled demand can be equally or even more predictable than scheduled demand (Walley et al. 2016; Litvak et al. 2015). To cope with natural variability, the level of predictability for unscheduled demand allows for forecasting and planning of resources to some extent, thereby improving resource utilisation. Artificial variation as a result of poor nursing home practices can be reduced by eliminating these practices (Walley et al. 2016; Litvak et al. 2015), so it is important to identify the source of the variation. The Results show how the case studies revealed challenges such as SOP adherence, work conditions, employee retention and absenteeism, the physical constraints of the nursing home, the possible negative impacts of one process on related processes, communication challenges, collaboration with other staff groups, continuous education, excessive use of water, balancing priorities, locating people and items, control of the process, stock count accuracy and maintenance of central and decentral technologies. As reiterated by Towill and Christopher (2016), it is important to adopt a holistic approach to improve to avoid sub-optimisation. They reflect on Braess’ Paradox, which states that optimising one small part of a system may have a negative impact on the system as a whole. It is therefore important to consider the impact of any change on related processes.
Interventions
Interventions for improving healthcare logistics processes were identified in the literature review, provided in the case studies and reported in the Results. The identified interventions can be divided into four categories, representing changes to processes, logistics and SCM aspects, technologies and organisational aspects. The interventions can be perceived as elements of logistics processes in nursing homes and can contribute to characterising those processes. Thus, the process interventions describe aspects of the process design. The investigated process types are also the means of carrying out logistics activities, although it is the technologies and staff resources which actually perform the logistics activities. Each type of intervention is discussed below. BPM interventions. Some authors have argued that a process approach is difficult to adopt in a healthcare setting due to their complex environment and demand uncertainty (Aronsson et al. 2011; Lillrank et al. 2011). However, the literature review showed that BPM approaches have been successfully applied in healthcare logistics settings, including BPR, cellular operations, performance measurement, benchmarking and process standardisation. The case studies also included best practices such as reducing and controlling handovers to ensure control of the process and to reduce the risk of mistakes. Moreover, the healthcare logistics processes can be benchmarked by operationalising the identified impact factors. Another similarity between the literature and case studies was the continuous improvement approach characteristic of nursing homes. Lean projects were also carried out in the nursing homes, although not for the investigated processes in particular. Thus the process improvement approaches applicable in a healthcare setting may likely apply to healthcare logistics. One example is the application of lean in healthcare (Souza 2019), although lean in healthcare tends to focus on its tools and techniques rather than systemwide implementation (Radnor et al. 2006; Radnor et al. 2012). This finding by Radnor et al. 2006 is consistent with the findings of the literature review, which only reported how JIT had been implemented in healthcare logistics and not lean as a management philosophy. Furthermore, as complementary to lean, some authors argue for an agile or leagile approach to cope with variability in a healthcare setting (Rahimnia and Moghadasian 2010). Lean and other management philosophies are based on quality approaches such as TQM, which studies have shown is applicable in a healthcare setting (Xiong et al. 2015; Smith and Offodile 2008). An alternative quality-related approach applicable in a healthcare setting is six sigma (Taner et al. 2017), although a survey of patient logistics in nursing homes showed that it was one of the least-implemented improvement approaches (van Lent et al. 2012, achieving a six-sigma quality level may prove difficult for healthcare logistics processes due to the nature and frequency of the processes. Logistics and SCM interventions. The logistics interventions identified in the literature review related to either replenishment systems or SC design. Interventions related to replenishment systems include replenishment policy, JIT and stockless systems, while those related to SC design included SC integration, SC and logistics innovation and responsive SCs. For the case studies, the replenishment policy was represented through the use of reorder points. Furthermore, the decentralisation and centralisation of both activities and inventories were significant differences identified between the case studies. Closely related to inventories was the concept of decoupling points (Rahimnia and Moghadasian 2016). Towill and Christopher (2015) considered decoupling points for patient flows, as they can ensure that different pipelines of healthcare delivery do not interfere with each other, thereby avoiding disruptions. Similarly, decoupling points may be worth taking into consideration for healthcare logistics. The characteristics of each process, such as variability and volume, should then determine whether a given sub-process should be agile or lean. They also argued that the difference between lean and agile operations lies in the variability of lead times and capacity (Towill and Christopher 2015). Thus, a lean approach operates with fixed (planned) capacity and emphasises the high utilisation of resources. This leads to variability in lead or waiting times if demand fluctuates. An agile approach, however, operates with fixed lead times and flexible capacity, requiring the high availability of extra resources (Aronsson et al. 2016). Modig and Åhlström (2013) discussed the concept of efficiency in relation to lean and distinguished between resource efficiency and flow efficiency. Resource efficiency focuses on the utilisation of resources and maximises value-added time as a resource, whereas flow efficiency focuses on the flow of a unit and maximises value-added time experienced by the unit. Lean is perceived as a strategy for increasing resource and flow efficiency within the natural limitations caused by variation. Designing a responsive SC was identified as an intervention in the literature. Callender and Grasman (2017) argued that a responsive SC might be better than an efficient cost-focused SC, although a responsive SC does not necessarily imply high inventory levels (Callender and Grasman, 2017). Their study found that one-third of healthcare providers experienced frequent emergency orders because of stock-outs. Responsiveness was not a particular issue in the case studies. In addition to the logistics and SCM interventions identified in literature, healthcare logistics processes might benefit from practices found in the manufacturing industry. SC models adopted from manufacturing may have to adapt to a service environment such as health care. However, Aitken et al. (2016) argued that both manufacturing and service industries struggle to achieve seamless supply chains and that there are more similarities than dissimilarities between service and manufacturing from an SCM perspective. Technological interventions. The applied technologies identified in healthcare logistics literature include automated transport, e.g. automated storage and retrieval, barcodes and RFID in general. Similar technologies were identified in the case studies, particularly washing machines and equipment to load and unload mattresses. However, other technologies could apply in a healthcare logistics setting, such as industries at the forefront of automation, particularly manufacturing. As an example, iBeacons were suggested by one interviewee at the primary case nursing home to direct relevant information to cleaning staff when they enter a room.
Benefits of Interventions
Which benefits can be identified for interventions and approaches for improving healthcare logistics processes? The literature review and the results of the study identified benefits for each intervention. In the literature review, the following nine types of benefits were identified: process performance and cost savings; quality; inventory management; flow management; safety; compliance; staff; procurement; and information management and SC coordination. The reasons for implementing the interventions were also identified to demonstrate how they related to the identified benefits, which in turn related to logistics, technologies, processes and organisational structure. Of the 24 identified impact factors, the identified benefits related to all but two impact factors: downtime and maintenance and utilisation of technologies. The benefits identified in the case studies were also shown to improve overall performance of logistics processes in terms of efficiency and effectiveness. As noted in the Introduction, cost containment and high-quality care are major concerns within healthcare (OECD 2015; WHO 2010; Saltman and Figueras 1997). Quality is reflected in the benefits identified both in the literature review and the case studies; those identified in the Literature Review and the Results related to costs in terms of efficient utilisation of resources. All of the nursing homes were required to provide economic justification for any potential investments in interventions.
Contingent Factors
What are the contingent factors which determine when different interventions and approaches for improving healthcare logistics processes are recommendable? Whether an intervention should be implemented depends on a number of contingent factors. The literature review identified 20 contingent factors relating to logistics and SCM interventions and 13 contingent factors relating to technological interventions. The following seven contingent factors were identified in the case studies: 1) Reorder points mainly applied to tangible items, rather than closed-loop flows; 2) trade-offs exist in terms of transport and lead time for the centralisation or decentralisation of activities; 3) centralisation vs. decentralisation of inventories depends on the centralisation or decentralisation of activities; 4) legal requirement and process control may provide incentives for implementing interventions; 5) the implementation of interventions depends on available financial resources; 6) nursing home size, the need to control processes, and the extent of available resources influence the decision to centralise or decentralise activities; 7) central inventories may be preferable for economic reasons. Comparing the contingent factors identified in the case studies and literature review, financial resources being identified as a contingent factor in the case studies is reflected in the contingent factor TCO discussed in the literature review (Pinna et al. 2015; Gebicki et al. 2014; Marino 1998). TCO was identified as a contingent factor related to logistics and SCM interventions but could apply to any type of intervention. Finally, tangibility was identified in the studies as a contingent factor related to reorder points and was identified in the literature review as a contingent factor for implementing a JIT solution (Whitson 1997).
Process Characterisation
How can healthcare logistics processes be characterised in terms of challenges and composite design elements? Pan and Pokharel (2017) provide a framework for characterising logistics activities in nursing homes to enable the design of a better system of delivering more efficient care services. The framework contains four aspects: 1) the nursing home profile; 2) inventory management; 3) motivators and barriers; and 4) alliances and outsourcing. In this study, healthcare logistics processes were characterised in terms of challenges and the constituent elements, i.e. the process steps, logistics and SCM aspects, implemented technologies and organisational structure. Comparing the characterisations in this study to those presented by Pan and Pokharel (2017), inventory management relates to logistics and SCM; motivators and barriers relates to implemented technologies; and alliances and outsourcing relates to organisational structure. The two approaches differ with respect to including the nursing home profile and process steps. The benefits of interventions and contingent factors for interventions were identified in this study. The benefits of interventions identified in the literature review can be divided into nine different types, while those identified in the case studies relate to the impact factors identified in this study, except for downtime and the maintenance and utilisation of technologies. The contingent factors identified in the literature were only identified for logistics/SCM and technological interventions. Seven contingent factors were also identified in the case studies. Comparing the characterisation in this study to that of Aptel and Pourjalali (2016), the extent of responsibility given to logistics departments, the manner of distribution of supplies and the past efforts of improving the logistics function were also described in this study. However, amounts or volumes and the degree of partnerships between nursing homes and suppliers were considered to a lesser extent.
Impact Factors
The second RQ considered in this study was ‘Which factors should decision makers consider when improving healthcare logistics processes?’ This question was answered through two underlying SQs, which are discussed below.
Identifying Impact Factors
Which factors impact the design of healthcare logistics processes? Based on the case studies, 24 impact factors were identified. The Results show how the impact factors were identified, although not all of them apply to all types of healthcare logistics processes. Environmental considerations was found to be relevant for only one case study. The impact factors were identified based on challenges and reasons for implementing interventions in the case studies. Additional challenges and interventions were identified in the literature review. Some challenges and interventions were identified in both the case studies and the literature review, while others were only identified in one or the other. The challenges identified only in the literature review included lack of predictability, political agendas and high SC costs. The types of interventions identified only in the literature review included responsive SCs (i.e. a logistics and SCM intervention) , Two benefits, procurement and information management and SC coordination, were identified in literature but not identified in the case studies. 15 further decision criteria were identified in the literature review for selecting technologies. In addition to the impact factors identified in the case studies and the possible additional impact factors identified above, the following impact factors could be added for technologies in particular: Reductions in theft and wasted products, improved reverse logistics and improved information storage. Depending on the scope of the decision to be made, these impact factors may or may not be included in the decision process for improving healthcare logistics.
Impact Factors and Process Design
How do impact factors affect the design of healthcare logistics processes? The design of healthcare logistics processes can be understood as the combination of composite elements of a process, such as technologies, logistics and SCM aspects and organisational structure. Additional process steps can be introduced to improve the output quality of a process. In some nursing homes, washing machines have been introduced to increase the cleanliness of beds, i.e. the output quality. The literature review also provides examples of interventions designed according to impact factors. For instance, one nursing home implemented a seven-step cleaning process to ensure consistency, reduce the risk of mistakes, improve output quality and ensure competence match. Some impact factors are perceived as more important than others depending on the process. The relationships between the impact factors are important to consider when making changes in a healthcare logistics system. One of the identified relationships between impact factors is the effect of competence match on output quality. Competence shifts also impact the quality-related factors of risk of mistakes and consistency. The Results show how competence match and competence shifts affect quality, indicating that these impact factors should receive more attention than suggested by their low rankings as decision criteria. Although less automated than its US counterparts, the case study ranked degree of automation higher than the US case studies. However, the case studies showed that automation is not a goal in itself; a semi-automated solution may be preferable due to staff considerations, space availability and flexibility. In some cases, a manual process may even be preferable, such as in the case of patient transport. The differences in perceived importance of impact factors are outlined in the Results section. The five highest-ranking impact factors were output quality, consistency, employee engagement, risk of mistakes and security of supply. For the UK cases, risk of mistakes, output quality and employee engagement were the highest-ranking impact factors, while for the US cases patient care, experience and safety, compliance and consistency ranked highest. Information management and traceability also ranked highest for the US cases, which differed from the overall ranking. For the logistics cases, output quality, employee engagement and consistency were found to be of high importance, and information management, security of supply, employee engagement and risk of mistakes ranked high as decision criteria. These differences in the importance of impact factors should be considered when assessing potential changes to healthcare logistics processes. The differences suggest that contingencies such as country setting and process type are used to determine what is considered important for improving a process and consequently influence the preferred design of a healthcare logistics process. The quality and cost aspects of healthcare motivating this study are reflected in the impact factors, indicating that the impact factors of output quality, risk of mistakes and consistency all relate to quality. Other aspects of quality include lead time and security of supply. Furthermore, impact factors such as competence shifts, competence match and employee engagement affect the quality of provided services. With regard to costs, the efficiency-related impact factors all contributed to a better use of resources, thereby reducing and controlling costs. The decision criteria lead time, value-added time, risk of mistakes and output quality can also be viewed from a cost perspective. Moreover, the degree of automation and the elimination of unnecessary processes can increase process efficiency. Using the proposed framework as a decision tool to change healthcare logistics processes will therefore promote processes which are more cost-effective and quality-oriented.
Impact Factors
Which factors should decision makers consider when improving healthcare logistics processes? A set of 24 impact factors were identified in the case studies for improving healthcare logistics processes, and seven other factors were added based on the literature review. For technologies in particular, four impact factors were added based on the literature review. The impact factors were shown to impact the design elements of healthcare logistics processes, specifically the process steps, logistics and SCM aspects, technologies and organisational structure. Differences in the importance of the impact factors were identified for national settings and process types. The interrelations between impact factors should thus be considered when considering changes to a healthcare logistics system.
Assessment
The third RQ, ‘how can the identified impact factors be used to assess healthcare logistics systems?’, considered the assessment of potential solutions for healthcare logistics processes. This RQ was answered based on two sub-questions, each of which is discussed below.
Benchmarking and Performance Measurement
How can the identified impact factors be used to measure and benchmark the performance of healthcare logistics processes? Bourne et al. (2016) proposed that the use of performance measurement systems be divided into three main phases: design, implementation and use. In relation to the design of performance measures, a set of performance measures for the nursing home cleaning process. Furthermore, a set of performance measures based on the impact factors for the purpose of benchmarking. In terms of implementing performance measures and how the identified impact factors can be used for assessing technologies which enable data capturing and performance measurement. This assessment is part of the implementation phase proposed by Bourne et al. (2017), in which data collection is enabled to produce regular performance measurements. The final stage of designing a performance measurement system, the use of performance measures, was not addressed in this study. The performance measures proposed were developed based on the highest-ranking impact factors and thus relate to quality, security of supply, employee engagement, customer satisfaction and lead time. However, identifying performance metrics was not the main purpose of this paper. Although benchmarking and performance management both consist of performance metrics, the two concepts are distinctly different from each other. Performance measurement can be defined as ‘the process of quantifying the efficiency and effectiveness of action’ (Neely et al. 2015). Accordingly, each of the impact factors were divided into efficiency- and effectiveness-related factors to reflect these performance aspects. Furthermore, the performance metrics developed related to improved service, quality and cost containment, which were the initial motivators of this study. The developed quality metrics thus related to both output quality (e.g. clean beds) and the timely delivery of services (e.g. lead time for transports and cycle time for cleaning). Finally, the cost aspect was represented by the efficiency aspect of performance measurement—in other words, the economic use of resources. Performance is multi-dimensional and multiple performance measures are therefore necessary to reflect performance (Chow et al. 1994). Chow et al. (1994) argued that logistics performance should reflect a set of goals and provide examples thereof; the goals considered in the case studies included job security and working conditions, customer satisfaction, product availability, cost-efficiency, social responsibility, on-time delivery, keeping promises and low rates of loss and damage (Chow et al. 1994). Korpela and Tuominen (2016) used the factors of reliability, flexibility, lead time, cost-effectiveness and added value for the purpose of benchmarking logistics operations. Each of these performance aspects are considered in this study. Flexibility was mentioned by both Chow et al. (1994) and Korpela and Tuominen (2016), but it was only considered to a limited extent in this research project. Wong and Wong (2018) defined benchmarking as a management tool which systematically searches for best practices, innovative ideas and efficiencies for continuous improvement purposes. Benchmarking can also be defined as consisting of both a best practice aspect and a performance metrics aspect (Voss et al., 1997; Camp 1989). Some best practices were identified in the Literature Review and in the Results, but they may differ according to the circumstances under which a nursing home operates—the best practices for one type of nursing home may not be as suitable for another. The framework developed in this study can serve as a decision tool for determining the most suitable solution given the circumstances of a nursing home, so the identified best practices should be considered a catalogue from which possible interventions can be assessed for possible implementation. Some of the challenges related to benchmarking healthcare logistics SCs were addressed above. The quantification of impact factors according to the importance for improving healthcare logistics processes addressed the issue of differences in importance of performance measure across organisations (Simatupang and Sridharan 2014), country borders (van Lent et al. 2015) and contexts (Sousa and Voss 2001, 2018). The framework developed in this study takes these differences into account by enabling decision-makers to prioritise each aspect of the framework in the decision process. The benchmarking method developed can be used to benchmark healthcare logistics processes across nursing homes. However, benchmarking healthcare logistics processes against logistics processes in other industries such as manufacturing, might provide useful insights for improvement potential. Camp (1995) distinguished between four different types of benchmarking: internal, competitive, functional and generic. Internal benchmarking provides the least potential, while generic process benchmarking (regardless of process type or industry) provides the highest potential, although it is difficult in practice. Looking outside the healthcare industry could therefore provide useful learning points for healthcare logistics managers. In addition to using the impact factors as performance metrics, the impact factors could be applied as a type of balanced scorecard. In a balanced scorecard, the financial, customer, internal business process and innovation and learning perspectives are balanced (Kaplan and Norton 1992). Brewer and Speh (2016) developed an SCM balanced scorecard consisting of end customer benefits, SCM goals, SCM improvement and financial benefits. Radnor and Lovell (2013) justified the use of balanced scorecards in the UK healthcare setting. The framework developed in this study is quite different from a balanced scorecard, given that it considers the matters of logistics, technology, procedure and structure, but these four aspects and their underlying impact factors should be balanced according to the prioritisation of impact factors. One way to balance the four perspectives is by applying quantitative methods such as ANP and AHP to assess different solutions. Applying the impact factors as part of an assessment tool is discussed below.
Selecting the Best Solution
How can healthcare logistics processes be assessed to ensure a solution which best fits the preferences of a nursing home? Nursing homes often do not achieve their goals with regard to logistics and SCM interventions in healthcare, so managers must often rely on their own experiences and judgment when selecting an improvement approach (Volland et al., 2016; Romero and Lefebvre 2015; van Lent et al. 2012). The framework developed in this study, which consists of six steps and allows for qualitative and quantitative assessments of alternative interventions, enables managers to select the intervention most suitable for the needs and preferences of their facility. The framework also provides limited guidance as to selecting which process to improve, although it may highlight areas which need improvement by identifying major challenges or prioritising impact factors. Other studies have provided more guidance on selecting processes for improvement (see, for example, Davenport 2013, and Hammer and Champy 2013). The catalogue of practices identified in the literature and in the case studies provides a list of interventions for potential assessment. The developed framework narrows down possible alternatives, based first on the contingent factors and subsequently on the application of the impact factors, to find the most suitable solution according to a nursing home’s needs and preferences. The use of multiple decision criteria allows for the assessment of solutions by simultaneously considering different aspects of the solution. The importance of these aspects may differ across nursing homes depending on the environment in which they operate, their strategies and other contingent factors. ANP is one method for prioritising different alternatives based on a comparison of decision criteria in relation to these alternatives. Applying the ANP method allows for a quantitative assessment of solutions whilst taking the interdependencies between decision criteria into account (Saaty 2014a). A simpler method would be the application of the AHP method, and an even simpler method would be the weighted factor model (Meredith and Suresh 1986). Similar applications include Korpela and Tuominen’s model (1996), which benchmarked logistics operations by applying the AHP method to a set of critical success factors. Alternatives or complementary approaches to an analytic method are economic or strategic justification (also called descriptive justification) (Meredith and Suresh 2016). Providing a qualitative or descriptive account of each of the impact factors in relation to alternative solutions could provide more nuance and enhance the analysis. A particular aspect of assessing alternative solutions is the assessment of technologies. Technologies are assessed as part of a process design rather than in isolation. Track-and-trace technologies are assessed in terms of their ability to capture and provide valid data. Factors which put the data validity at risk were thus identified impacting the selection of a suitable technology. The purpose of technology assessment methods is to inform policymakers about the impact of a new technology. Health technology assessment in particular informs policymakers about technologies which solve health problems and improve the quality of life (Ritrovato et al. 2015; WHO 2015). The purpose of assessing technologies in this study is therefore more aligned with technology justification (Meredith and Suresh 1986).
Assessment
The impact factors identified in this study can be used for performance measurement and benchmarking purposes. The quantitative ranking of impact factors enables the identification of the most important impact factors and hence the most suitable aspects to be considered in performance measurement and benchmarking. The other aspect of assessment in which the impact factors can be applied is the evaluation of alternative interventions in healthcare logistics. A framework was developed for assessing alternative solutions using multiple decision criteria methods. The context of a nursing home, and subsequently the ranking of the impact factors, enables the selection of an intervention which reflects the needs and preferences of the nursing home. How can nursing home improve their logistical processes to ensure that the process design and performance fit the needs and preferences of a nursing home? According to Böhme et al. (2016), the literature provides little guidance on which interventions are most effective for certain situations. The interventions identified in the literature review and case studies may only be applicable under certain circumstances and provide the best results only under particular conditions. Contingency theory states that contingent factors determine the success and impact on performance of implementing best practices (Sousa and Voss 2018); it assumes that the context determines which OM practice or intervention should be implemented. In a way, contingency theory restricts the practices which can be chosen. Sousa and Voss (2018) distinguished between three types of variables in contingency theory: contextual variables, response variables and performance variables. Contextual variables can be further divided into four types of variables: national context/culture, firm size, strategic context and other organisational context variables. The contextual variables are usually exogenous and either cannot be controlled or can be controlled only to a limited extent. The ‘needs and preferences’ as expressed in the research question are determined by the contextual variables. A solution which fits the ‘needs and preferences’ of a nursing home is one which corresponds to the best fit between the contextual variables and response variables according to the performance variables. In an OM setting, process type is considered a contextual variable (Sousa and Voss 2018)—for example, in logistics, nursing home cleaning and distribution. The contingency factors identified in this study correspond to a type of contextual variable outlined in the contingency theory. The response variables are organisational or managerial activities undertaken in response to the contextual variables (Sousa and Voss 2018). In the case studies, the response variables were the identified interventions: BPM interventions, logistics and SCM interventions, technological interventions and organisational interventions. The last type of variable in contingency theory is the performance variable. Performance variables explain the selection of interventions or OM practices by evaluating the fit between contextual variables and response variables, and thus correspond to the impact factors identified in this study. Some impact factors, such as performance variables, were found to be relevant only for certain process types and national contexts. Furthermore, differences in the perceived importance of the impact factors were identified in the case studies. These perceived differences suggest that the nursing homes had different primary concerns depending on their particular context, e.g. country setting and process type. These differences in perceived importance fit well with the underlying assumption of contingency theory that the success of practices or interventions is context-dependent. In selecting practices or interventions to be implemented this study advocates a systems approach in which all contingencies, response variables and performance variables must be considered simultaneously (Sousa and Voss 2018). The framework developed in this study supports this approach by considering the context, interventions and impact factors and their interdependencies at the same time.
Limitations
This study is not without limitations. The domain limitations outlined in the Literature Review and the Methodology limited the focus of this study, and in terms of the investigated case studies the national context is limited to a logistics setting. Moreover, the case study nursing homes investigated were all private. Only three types of healthcare logistics processes were investigated (logistics, cleaning and HR), so the domain of the study focused primarily on the flow of materials—that on patient flows was limited. The distribution of services was included in the domain, as exemplified by the nursing home cleaning case. Other types of flows, such as staff flows and reverse flows, were not considered. The SC focus of this study was mainly on internal SC, with limited focus on the link to the first-tier supplier. The field of procurement was therefore not a focus of this study but was included solely in relation to replenishment activities. Areas such as telemedicine and outsourcing were also not explored due to the main focus being nursing home facilities. In terms of methodology, the use of quantitative methods was limited. Methods related to route optimisation, forecasting and scheduling were not included. The quantitative methods applied in the study were limited to the ranking of impact factors based on a small population of respondents. One of the limitations related to ranking is that the same type of ranking was not provided for all processes—for instance, the impact factors were not ranked for the nursing home cleaning case and the ANP method was used to rank the impact factors . The catalogue of interventions provided in this study was limited to the interventions reported in the literature and identified in the case studies. The rapid development of technologies and developments within research and other industries in the fields of BPM, logistics and SCM and organisational management will at some point render the catalogue of interventions obsolete, so interventions will need to be updated regularly to remain practical. The types of investigated interventions were limited to interventions related to BPM, logistics and SCM, technologies and organisational structure. Other types of interventions, such as those related to culture, leadership styles and financial incentive programs, were not included. The reasons for implementing such a systems from a logistics point of view was addressed in the framework, but the developed framework cannot provide complete and conclusive decisions regarding such a complex issue. However, the framework could serve as a small part of such a decision process. The validity of the findings of this study depends on the capabilities of the respondents. Callender and Grasman (2016) found that almost half of the respondents they surveyed (42.8 per cent) felt that executive managers had the required skills and knowledge to deal with SCM. The impact factors identified in this study were ranked by managers engaged in the investigated processes. The validity of the ranking of impact factors therefore depended on the capabilities of the managers and their ability to link the impact factors to the overall strategy of the nursing home and their knowledge of what is best for the nursing home from a logistics perspective. Suggestions for future research are provided in the concluding chapter.
Chapter Summary
This chapter answered and discussed the research questions investigated in this study. Healthcare logistics processes were characterised in terms of challenges and their composite elements, i.e. process steps, technologies, logistics and SCM aspects and their organisational structure The application of the impact factors in a decision process was discussed in terms of benchmarking, performance measurement and the assessment of possible interventions. Finally, the research question was answered and discussed in relation to contingency theory.
Conclusions and Future Research
This chapter concludes this study and offers suggestions for future research. The chapter is structured as follows: First, the research questions are answered in the concluding remarks; an account of the contributions to research is provided, followed by an assessment of the practical implications of the study; and finally a chapter summary is provided.
Concluding Remarks
The rising costs of healthcare provision and the increasing demand for high-quality care at a reasonable cost provided the initial motivation for this study. Logistics processes offer significant potential for cost reductions in nursing homes and are the focus of this research. A series of case studies at five UK nursing homes and one US nursing home was conducted to examine the logistics process in a nursing home setting. A case study of the cleaning process was then carried out at the primary nursing home, followed by a study of the HR process at the same facility. Two case studies were then conducted at the US nursing home to investigate the logistics and HR processes. The findings from the case studies were used to answer the research questions. Each of these research questions is answered below.

The research question was ‘how can nursing homes improve their logistical processes to ensure that the process design and performance fit the needs and preferences of a nursing home?’ It was answered through three subsidiary RQs and their underlying SQs, as explained below.
RQ1: How can healthcare logistics processes be characterised in terms of challenges and composite design elements?
Healthcare logistics processes were characterised in terms of challenges and their constituent elements in terms of process steps, logistics and SCM aspects, implemented technologies and organisational structure. Nine types of benefits across the different types of interventions were identified. The benefits of interventions identified in the case studies were reflected in the impact factors identified in this study, except for the impact factors of downtime and the maintenance and utilisation of technologies. The contingent factors determining the circumstances under which implementation of possible interventions is suitable were identified in the literature. The identified contingent factors were only identified for logistics/SCM and technological interventions in the literature review. Seven contingent factors were also identified in the case studies.
RQ2: Which factors should decision-makers consider when improving healthcare logistics processes?
Based on the case studies, 24 impact factors were identified which should be considered when improving healthcare logistics processes. The identified impact factors influence the design of healthcare logistics processes in terms of four constituent elements: process steps, logistics and SCM aspects, technologies and organisational structure. The impact factors were ranked according to their importance for improving healthcare logistics processes. Differences in the importance of impact factors were identified for specific process types and country settings. The case studies suggested a number of interrelations between the impact factors. When implementing interventions, these relationships should be considered to understand the impact on the system. Based on literature, an additional seven impact factors were identified, and a further four impact factors could be added for technologies based on the discussion of literature.
RQ3: How can the identified impact factors be used to assess healthcare logistics systems?
A framework was developed to assess alternative interventions. The framework consists of six steps and enables managers to select the intervention most appropriate for the circumstances in which their nursing home operates. A methodology for benchmarking healthcare logistics was proposed and suggestions for performance measures provided. The overall RQ investigated in this study was answered through the subRQs above. The challenges were identified, a catalogue of interventions was provided, and a framework to assure best fit of a solution for a nursing home has been developed. However, the findings of this study are subject to limitations, the most significant of which are the limited types of processes for which this study was conducted (logistics, cleaning and HR) and the limited country settings where the case studies took place (the United Kingdom and the United States).
Contributions to Research
The contributions this study makes to this field of research are presented below. Each contribution relates to improving healthcare logistics processes.
Enfolding of literature. The first contribution of this thesis was the establishment of the state of healthcare logistics literature. The literature in this field was explored and four themes identified: 1) BPM; 2) logistics and SCM; 3) technologies; and 4) organisational structure. Each of the identified interventions for improving healthcare logistics processes relates to one of the four identified themes. A synthesis of what literature has to offer in terms of improving healthcare logistics processes was provided, and an agenda for future research was developed based on the literature review.
Empirical evidence. Empirical evidence for improving healthcare logistics processes was provided in both the literature review and the case studies. Thus, the empirical evidence supports existing knowledge and provides new insights as to how to improve healthcare logistics processes.
Identification of challenges. Challenges inherent to logistics processes in nursing homes were identified based on extant literature and the conducted case studies. The identification of challenges allows for addressing those challenges through interventions.
Catalogue of interventions. Different types of interventions were identified and classified based on the literature and case studies. The types of interventions considered in this study related to BPM, logistics and SCM concepts, technologies and organisational structure. The benefits of each intervention were also identified.
Set of impact factors. A set of impact factors for improving healthcare logistics processes were identified based on the case studies and ranked according to their importance for improving healthcare logistics processes. In addition, the relationships between impact factors were suggested based on the case studies. Additional suggestions for impact factors based on the literature were provided in the Discussion.
Framework. A framework was developed for improving healthcare logistics processes. This framework is both theoretically and empirically grounded and can serve as a tool for assessing suitable interventions to improve healthcare logistics processes. The framework allows managers to make informed decisions while taking the context of the nursing home into account.
Filling the research gap. This study contributes to the limited field of healthcare logistics research. Within the healthcare logistics domain, this study contributes to four different streams of literature: BPM literature, logistics and SCM literature, technology assessment and justification literature and human factors and organisational management literature. The literature review revealed the gaps in healthcare logistics literature and this study is an attempt to fill part of that research gap. Regarding BPM literature, this study particularly contributes to the aspects of performance measurement, benchmarking and continuous improvement. Regarding logistics and SCM literature, a method was developed to assess the design of the internal SC. Furthermore, a method for assessing and justifying the implementation of technologies in a healthcare logistics process is provided. Finally, in relation to the organisational aspect, metrics for measuring staff performance were developed and the importance of employee retention and employee absenteeism for the quality of healthcare logistics processes was emphasised.
Practical Implications
Given the research aim to ‘provide theoretically and empirically based evidence for improving healthcare logistics processes […]’, this begs the question: What should practitioners do differently now? The practical implications of this study are therefore discussed below. First and foremost, this study provides a framework for managers to make informed decisions to improve healthcare logistics processes in nursing homes. A list of the main challenges in healthcare logistics processes is provided, which can help managers identify challenges inherent to their processes and help focus attention on any improvement efforts. To address challenges and help improve healthcare logistics processes in general, a catalogue of interventions is provided. Based on this catalogue of interventions, decision-makers can identify the most suitable improvement interventions given the circumstances of a specific nursing home. The circumstances under which to implement changes, i.e. the contextual variables, are provided to guide the decision. Thus, the identified contingent factors can help managers narrow down the number of interventions relevant to the situation of the manager. The findings of this study provide insights about the factors impacting the design of healthcare logistics processes—or, in other words, the selection of interventions to be implemented in a healthcare logistics process. The ranking of the identified impact factors as decision criteria enables context-specific decision-making based on the developed framework. Based on the ranking of impact factors as decision criteria, managers can prioritise interventions according to a list which has already been narrowed down based on the contingent factors. The ranking of impact factors as decision criteria may differ across nursing homes, but the findings of this study suggest that patterns exist for certain types of processes. The prioritisation of impact factors provided in this thesis can help managers determine where to focus their improvement efforts. The identified impact factors can help managers think about and determine whether their own priorities may differ from those identified in this study. Priorities may be specific to a particular process or a nursing home, which the framework addresses. Furthermore, the suggested interrelations between impact factors can help managers understand the implications of interventions and view healthcare processes holistically as part of a system. The ranking of impact factors provides another application for them—namely, benchmarking. The ranked impact factors enable the provided methodology to be used for benchmarking and measuring the performance of healthcare logistics processes.
Suggestions for Future Research
The suggestions for future research are based on the literature review and the limitations of this study.
The Research Agenda Emerging from the Literature Review
Although this study contributes to filling part of the gap identified in the literature review, much research is still needed to fully understand each of the aspects of this gap.
Methods. The most prevalent research method applied in the reviewed healthcare logistics literature is the case study method. Other literature reviews have focused on quantitative studies of the field (Dobrzykowski et al. 2014), which in turn have focused on mathematical modelling. More research is needed using surveys or mixed method approaches. However, given the maturity of the field, more qualitative research may be needed to form hypotheses to be tested through statistical analyses.
Clear definitions. Concepts such as JIT, stockless and VMI solutions need clear definitions in healthcare logistics literature, as there seems to be some disagreement on the matter.
BPM. Particular opportunities for future research include the investigation of process types other than the distribution of pharmaceutical products, blood products and sterile supplies. More research is needed on BPM, particularly for approaches and tools not reported in the literature of the field, such as TQM and lean.
Logistics and SCM concepts. Logistics and SCM together with technologies in healthcare logistics are the most investigated themes identified in the reviewed literature. Logistics and SCM topics such as SC integration and logistics and SC innovation have received little attention in the literature. Other logistics concepts not investigated in the field such as agile, lean and leagile SCs could provide opportunities for future research.
Technologies. In terms of technologies, the full potential of RFID and the potential applications of new types of technologies have yet to be explored in the field and would provide novel opportunities for research.
Organisational aspects. The least researched topic covered in this thesis was the organisational aspects of healthcare logistics, which offers rich opportunities for future research. The exploration of the human component in particular is much needed in the field (Stanger et al. 2012).
Interdisciplinary research. The interdisciplinary nature of this field calls for more research combining theories from various other research fields.
Contingent factors. The identified contingent factors mainly relate to logistics and SCM and technological interventions. Thus, contingent factors should be identified for other types of interventions.
Benefits. The benefits of each type of intervention should be mapped more extensively by considering literature outside the healthcare logistics field.
Learning from other industries. The field of healthcare logistics could learn from other fields which are further ahead in terms of process design and process performance.
To implement interventions. The change management aspect is important to ensure buy-in from logistics staff and other parts of the organisation. Change management may already be considered in the decision to select interventions to be implemented. Features and ease of use are considered in the developed framework, but other aspects could be beneficial to consider at an early stage to ensure the successful implementation of an intervention.
Applying quantitative methods. The findings of this study are suitable to be tested using more quantitative methods, particularly with regard to three aspects. First, the suggested interdependencies between impact factors identified in this study need further validation, and the suggested correlation between impact factors could be tested as hypotheses using statistical analysis. Second, the additional impact factors identified in the literature should be ranked alongside the impact factors identified in the empirical study. Third, the identified impact factors should be ranked based on a larger sample population.
Chapter Summary
This chapter summarised the findings of the study by answering each of the investigated research questions. The contributions to research were subsequently explicated and an assessment of the practical implications of the findings of this study provided. Suggestions for future research were offered based on both the conducted literature review and the empirical study.
Reflections
In this brief concluding section, the author’s reflections on the research conducted in this study are offered, including opinions, ponderings, surprises and hopes for the future of the field of healthcare logistics. Most of the fieldwork conducted in this research project was conducted at the main UK case study nursing home. During the course of the project, regular meetings were held with the logistics managers of the facility to make sure the project stayed on track. Additional reports were provided as a part of the case study, along with recommendations on how to address the facility’s immediate challenges. It is to be expected that such reports, recommendations and support for the organisation will be conducted during the research done as part of a PhD, although these aspects may not be a direct part of the research outcome. It is thus the responsibility of organisation being studied to decide which recommendations they wish to implement once the researcher as no further association with their operations. As noted by Creswell (2015), research consists of posing a question, collecting data to answer the question and finally presenting an answer to the question. Unfortunately, none of the recommendations were implemented in the facilities studied during the course of this research, which could be attributed to a number of reasons. First, the nursing home experienced a change in management, and so the new staff were not part of the initial framing of the research project and ongoing discussions. Second, as experienced by several private institutions, financial concerns were a constraint on their involvement, and some of the recommendations required an investment which these facilities were not in a position to make. Third, other projects were ongoing in the nursing home regarding the possible implementation of RFID, although no definitive decision was made, nor were guidelines for future use provided. Fourth, the nursing home was in the midst of adding a new building to its premises, which would ultimately dictate the design of the future supply chain and logistics processes within the facility. It is to be hoped that the nursing home will utilise the knowledge gained from the research project to improve their logistical setup, but circumstances did not seem to be in favour of such developments at the time of writing. The research outcome of this project was useful to the managers and suggests further research and implementation of practices which could be applied in a nursing home healthcare setting. During the time spent at the facility to conduct fieldwork, the author not only had the opportunity to investigate the case study processes but also to learn about the UK healthcare system, particularly the continuous improvement and operational excellence which were integral to the nursing homes’ operation. I also had the opportunity to provide support in ongoing projects, which helped me understand how to improve not only logistics processes in nursing homes but processes in general, including administrative tasks. The external research provided a better understanding of how healthcare systems in other countries work, especially a country whose healthcare system is often referred to both in academia and the industry.
One surprising aspect of the research findings was the importance of organisation and human resources to the findings of this study. Initially, the focus of this research project was more on technologies but shifted into a broader consideration of improvement efforts. Further surprises were that the research field of healthcare logistics is relatively limited and that logistics processes in nursing homes lag far behind those of the manufacturing industry. Nursing homes could learn a lot by sharing knowledge and benchmarking within and across industries and country borders. Hopefully, nursing home logistics will receive the attention it deserves and be recognised by other industries as an area of strategic importance rather than merely being viewed as a costly part of business. Fortunately this change in perception does seem to be underway. The focus in society on the provision of quality care while reducing costs provides a good incentive for further research in terms of what the operations management field can offer, not only for logistics processes but for any aspect of nursing home operations. Continued research in the field is therefore both expected and will be useful in providing affordable, high-quality care. Doing a PhD has been an immense privilege for me and I am grateful to have had the opportunity to spend three years delving into such an interesting research topic. It is my hope that the findings of this research project will result in better-quality and cost-effective healthcare logistics processes.
References
Peters, A., Otter, J., Moldovan, A., Parneix, P., Voss, A. and Pittet, D., 2018. Keeping hospitals clean and safe without breaking the bank; summary of the healthcare cleaning forum 2018.
Pohjosenperä, T., Kekkonen, P., Pekkarinen, S. and Juga, J., 2019. Service modularity in managing healthcare logistics. The International Journal of Logistics Management.
Brax, S.A., Bask, A., Hsuan, J. and Voss, C., 2017. Service modularity and architecture–an overview and research agenda. International Journal of Operations & Production Management.
Grol, R., Wensing, M., Eccles, M. and Davis, D. eds., 2013. Improving patient care: the implementation of change in health care. John Wiley & Sons.
Pittet, D., Allegranzi, B., Sax, H., Dharan, S., Pessoa-Silva, C.L., Donaldson, L. and Boyce, J.M., 2006. Evidence-based model for hand transmission during patient care and the role of improved practices. The Lancet infectious diseases, 6(10), pp.641-652.
de Vries, J., Huijsman, R., Aronsson, H., Abrahamsson, M. and Spens, K., 2011. Developing lean and agile health care supply chains. Supply chain management: An international journal.
Kilpatrick, C., Storr, J. and Allegranzi, B., 2017. Hygiene in Healthcare Campaign. Hand hygiene: a handbook for medical professionals, 9, p.275.
Quintana, J.M., González, N., Bilbao, A., Aizpuru, F., Escobar, A., Esteban, C., San-Sebastián, J.A., de-la-Sierra, E. and Thompson, A., 2006. Predictors of patient satisfaction with hospital health care. BMC health services research, 6(1), p.102.
Schoenfelder, T., Klewer, J. and Kugler, J., 2011. Determinants of patient satisfaction: a study among 39 hospitals in an in-patient setting in Germany. International journal for quality in health care, 23(5), pp.503-509.
Mitchell, B.G., White, N., Farrington, A., Allen, M., Page, K., Gardner, A., Halton, K., Riley, T.V., Gericke, C.A., Paterson, D.L. and Graves, N., 2018. Changes in knowledge and attitudes of hospital environmental services staff: the researching effective approaches to cleaning in hospitals (REACH) study. American Journal of Infection Control, 46(9), pp.980-985.
de Rezende, B.A., Or, Z., Com-Ruelle, L. and Michel, P., 2012. Economic evaluation in patient safety: a literature review of methods. BMJ quality & safety, 21(6), pp.457-465.
Strassle, P., Thom, K.A., Johnsonm, J.K., Leekha, S., Lissauer, M., Zhu, J. and Harris, A.D., 2012. The effect of terminal cleaning on environmental contamination rates of multidrug-resistant Acinetobacter baumannii. American journal of infection control, 40(10), pp.1005-1007.
Mann, E.E., Manna, D., Mettetal, M.R., May, R.M., Dannemiller, E.M., Chung, K.K., Brennan, A.B. and Reddy, S.T., 2014. Surface micropattern limits bacterial contamination. Antimicrobial resistance and infection control, 3(1), pp.1-9.
Bal, L., 2015, October. SiP Drivers and Challenges: Supply Chain Outlook and Requirements. In International Symposium on Microelectronics (Vol. 2015, No. S2, pp. S1-S21). International Microelectronics Assembly and Packaging Society.
Min, H., Joo, S.J. and Nicolas-Rocca, T.S., 2016. Information system outsourcing and its impact on supply chain performances. International Journal of Logistics Systems and Management, 24(4), pp.409-425.
Xiong, J., He, Z., Ke, B. and Zhang, M., 2016. Development and validation of a measurement instrument for assessing quality management practices in hospitals: An exploratory study. Total Quality Management & Business Excellence, 27(5-6), pp.465-478.
van Lent, W.A., Sanders, E.M. and van Harten, W.H., 2012. Exploring improvements in patient logistics in Dutch hospitals with a survey. BMC health services research, 12(1), p.232.
Rahimnia, F. and Moghadasian, M., 2010. Supply chain leagility in professional services: how to apply decoupling point concept in healthcare delivery system. Supply Chain Management: An International Journal.
Towill, D.R., 2006. Viewing Kaiser Permanente via the logistician lens. International Journal of Health Care Quality Assurance.
Callender, C. and Grasman, S.E., 2010. Barriers and best practices for material management in the healthcare sector. Engineering Management Journal, 22(4), pp.11-19.
World Health Organization, 2010. The world health report: health systems financing: the path to universal coverage: executive summary (No. WHO/IER/WHR/10.1). World Health Organization.



- 24/7 Customer Support
- 100% Customer Satisfaction
- No Privacy Violation
- Quick Services
- Subject Experts